💥 New review from @TheLancet on Dx of #CAD.
👉 Bottom line: The field continues to shift toward plaque-centric #CCTA, with functional tests layered on for ischemia, reflecting a more comprehensive approach to chronic CAD.
www.thelancet.com/journals/lan...
@drmarthagulati.bsky.social #CardioSky
04.12.2025 00:32 — 👍 0 🔁 0 💬 0 📌 0
www.jacc.org/doi/epdf/10....
@CardioOnc_MR_CT @RonBlankstein @hahn_rt
@ACCinTouch @American_Heart @SCCTorg @SCMRorg
#cardioSky
19.11.2025 00:02 — 👍 0 🔁 0 💬 0 📌 0

🔥 Hot off the press! 2025 CV Imaging Training Statement
🛣️ New "Advanced Imager" pathway with Level II-like competence in CT, MR, Echo, and Nuc
🚀 Nice emphasis on cross-modality integration for CAD, sarcoid, amyloid, HCM pericardium, masses, structural, and ACHD
Link below👇
19.11.2025 00:02 — 👍 0 🔁 0 💬 1 📌 0

🚨 New AHA statement on NOCA from @CardioMDPhD @lesleejshaw and others.
👉 AI plaque analysis improves risk discrimination and changes downstream management.
🚀 @NorthwellHealth will be studying this as we prepare to roll out Plaque Analysis!
#CardioSky
www.ahajournals.org/doi/10.1161/...
11.11.2025 23:00 — 👍 0 🔁 0 💬 0 📌 0
👧 Family: ECG+echo (CMR if equivocal); echo q1–2y, CMR q2–5y
🧩 Phenocopies: Amyloid (EF/GLS >4.1, high T1), Fabry (low T1, basal IL LGE), Athlete (balanced dilation, no LGE)
🤖 Future: AI, indexed wall thickness, DTI/FAPI
doi.org/10.1093/ehjc...
#CardioSky
07.11.2025 00:33 — 👍 0 🔁 0 💬 0 📌 0
🚦 Obstruction is dynamic: LVOTO >30 rest, >50 provoked
⏳ Mid-cavity HCM = hourglass LV & apical aneurysm; doppler underestimates pressures
🌫️ Ischemia w/o CAD is common: check CMR/PET for microvascular dysfunction
💊 Therapy monitoring: CMIs: start for EF ≥55–60%; hold <50%
07.11.2025 00:33 — 👍 0 🔁 0 💬 1 📌 0
🧭 Diagnosis ≠ MWT ≥15 mm alone: use phenotype, function, tissue characterization
🔥 LGE matters: ~65% have LGE; ≥15% LV mass can up-class ICD risk
🎯 EF can mislead: track GLS for systolic dysfunction
🫁 Diastolic assessment: EACVI/ASE 4-criteria + LA strain; exercise echo
07.11.2025 00:33 — 👍 0 🔁 0 💬 1 📌 0

🚀 New #EACVI consensus statement on multimodality imaging for #HCM from @s_e_petersen @cardim_nuno. #Echo, #CMR, #CCT, and #PET each add unique value across diagnosis, symptoms, prognosis, screening, and treatment monitoring.
Key points👇
07.11.2025 00:33 — 👍 1 🔁 1 💬 1 📌 0
🚀 CT perfusion can provide volumetric MBF maps that pair seamlessly with #CCTA for a single comprehensive exam. ?Could this offer a one-stop shop?
doi.org/10.1016/j.jc...
#cardiacimaging #cardioSky
04.11.2025 23:00 — 👍 0 🔁 0 💬 0 📌 0
🧱 Historically, there has been limited access to PET scans needed to quantify MBF. But this is changing.
👏 As described in this expert review, CT & MRI are now validated to deliver comprehensive/actionable reporting on MBF, bringing greater precision to the chest pain pathway.
04.11.2025 23:00 — 👍 0 🔁 0 💬 1 📌 0

💥 Myocardial Blood Flow (#MBF) isn't just a #PET thing anymore. #CCT and #CMR are in the game.
🚦 Angina isn't always explained by epicardial stenoses. Quantification of MBF can detect other causes (#ANOCA), like microvascular disease, HCM, or transplant vasculopathy.
04.11.2025 23:00 — 👍 0 🔁 1 💬 1 📌 0
🚀 If we start reporting even 3 of these opportunistic metrics (e.g. RV function, membranous septum length, frailty marker), we move CT-TAVR from procedural planning → phenotyping platform.
#TAVR #StructuralHeart #cardioSky @danilorenzatti @CardioMDPhD
30.10.2025 23:33 — 👍 0 🔁 0 💬 0 📌 0
🔹 Frailty on CT: psoas/skeletal muscle index + vertebral HU → osteosarcopenia → worse 1-year outcomes.
🔹 CAD beyond “is there calcium?”: better CCTA (PCCT) + CT-FFR can reduce the number of patients we send for invasive angio.
30.10.2025 23:33 — 👍 0 🔁 0 💬 1 📌 0
🔹 Amyloid signal: CT-ECV (esp. with dual/spectral or photon-counting) → separates AS remodeling from coexisting ATTR, which is not rare in this population.
🔹 Fat: EAT / peri-coronary fat volume + attenuation → inflammatory signature that tracks with MACE after TAVR.
30.10.2025 23:33 — 👍 0 🔁 0 💬 1 📌 0
🔹 Conduction risk: membranous septum length, LVOT/root/mitral annular calcium → helps predict who’s heading for a PPM.
🔹 Myocardial phenotype: full-cycle CT → RV function (often missed on echo), CT-GLS, “cardiac damage” staging → all tied to mortality after TAVR.
30.10.2025 23:33 — 👍 1 🔁 0 💬 1 📌 0

We’re doing CT before most TAVRs, but we’re only cashing in on the “planning” part. This review argues we should be squeezing the rest of the dataset for prognosis and longitudinal care.
www.journalofcardiovascularct.com/article/S193...
What else is sitting on those scans? 👇
30.10.2025 23:33 — 👍 1 🔁 1 💬 1 📌 1

💥 Masterful review of the literature on CT-FFR in @journalCCT
www.journalofcardiovascularct.com/article/S193...
#CCTA + #CTFFR = anatomy + physiology in one stop 🚀
Growing evidence to look at the translesional ΔFFR, not just the distal FFR value 🔺
@PRodriguezMD #cardioSky #CAD #SCCT
29.10.2025 23:32 — 👍 3 🔁 1 💬 0 📌 0

🤔 Thought-provoking piece in @CircAHA from Kole & Joshi
🫀 A growing group of patients with subclinical atherosclerosis falls in between traditional "primary" and "secondary" prevention. I've heard of "prevention 1.5" or "plaque-informed prevention." How about the following classification system?👇
27.10.2025 22:21 — 👍 0 🔁 0 💬 0 📌 0
🌈 Spectral data paves the way for plaque phenotyping, perfusion mapping, myocardial characterization - a possible "one-stop" exam?
🤔 Still need: larger prospective clinical validation and cost-effectiveness data
📖 www.jacc.org/doi/10.1016/...
@ArthurShiyovich @RonBlankstein #cardioSky #CCTA
24.10.2025 22:50 — 👍 1 🔁 0 💬 0 📌 0


💥 Just out in #JACC CVI: State-of-the-Art on Photon-Counting CT
👇 Why this technology is a game-changer:
☢️ Better for patients: ⬇️ radiation and ⬇️ contrast
😅 Better for readers: spatial rez of 0.1mm + ⬇️ blooming = stents and calcified plaques are clearer than ever before
24.10.2025 22:50 — 👍 1 🔁 0 💬 2 📌 0
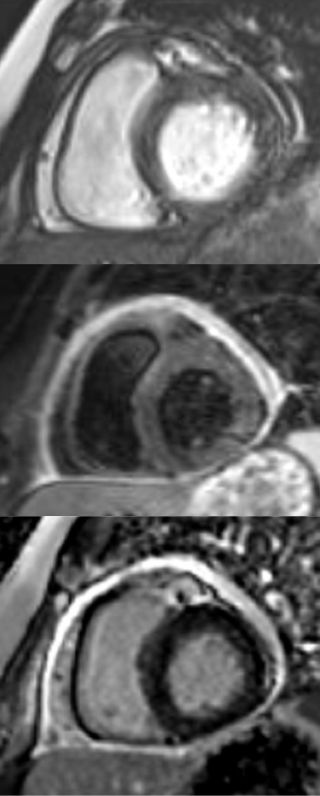
✨ Beautiful #CMR pictures. Young patient with new chest pain. SSFP, T2W, and LGE.
#NorthwellHealth #cardiosky
21.10.2025 22:00 — 👍 1 🔁 1 💬 0 📌 0
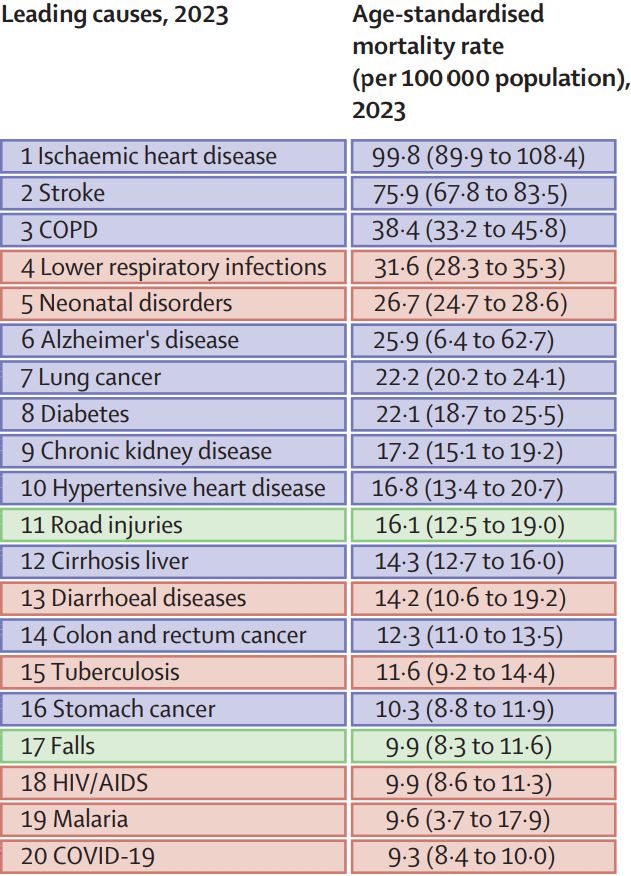
🪦 Ischemic heart disease remains the #1 cause of death worldwide
💥 That's 8.9M premature deaths or 136M years of life lost in 2023 alone
💊 We need a better strategy to detect and prevent ischemic heart disease
👏 Thanks to GBD for another incredible report: www.thelancet.com/journals/lan...
#CCTA
14.10.2025 23:02 — 👍 0 🔁 0 💬 0 📌 0
👉 Key strategies include: prospective gating, reduced field of view, BMI-tailored kVp, elimination of redundant phases, and hands-on training for techs.
🔬 Here, Chazal et al describe how a multicenter CCTA program used these strategies to lower mean radiation dose by 23%! doi.org/10.1016/j.ja...
14.10.2025 22:01 — 👍 0 🔁 0 💬 0 📌 0

💥 As coronary CTA volumes increase, we must keep radiation exposures as low as reasonably achievable.
☢️ AHA/ACC/SCCT recommend a goal of median CCTA dose ≤4 mSv, which has been achieved in multicenter trials without compromising quality.
14.10.2025 22:00 — 👍 0 🔁 0 💬 1 📌 0
❗ Impressively, only 1% of scans were indeterminate, and there was good diagnostic performance regardless of stent diameter.
@DoosupShin @ziadalinyc @OKhaliqueMD #cardiotwitter #CCTA
eurointervention.pcronline.com/article/phot...
09.10.2025 23:33 — 👍 0 🔁 0 💬 0 📌 0

💥 Photon-counting detector CT offers good diagnostic accuracy for detecting ISR, overcoming artifacts that have plagued prior generations of scanners.
🔬 In a blinded study of 283 stented lesions, PCD-CT, as compared to cath, demonstrated NPV of 96.4% and accuracy of 88.9% for ISR ≥50%.
09.10.2025 23:33 — 👍 0 🔁 0 💬 1 📌 0

🧲 #CMR can identify cardiac allograft vasculopathy effectively and non-invasively.
🔬 In this study of 110 patients s/p heart transplant, quant myocardial perfusion reserve <2.2 had NPV 100% and AUC 0.88 for significant CAV, as compared to cath. doi.org/10.1093/ehjc...
@SCMR @EHJ #CardioSky
08.10.2025 23:32 — 👍 0 🔁 1 💬 0 📌 0

Redefining the risk of major arrhythmic events in non-ischaemic cardiomyopathy: insights from the DERIVATE-NICM study
AbstractAims. Selection of the patients for implantable cardioverter defibrillator primary prevention therapy in non-ischaemic cardiomyopathy (NICM) needs
💫 #CMR is useful for predicting SCD in NICM.
📊 DERIVATE 2.0 provides better risk classification, incorporating gender, LVEF, and amount/location of #LGE.
👉 Let's look beyond LVEF alone to determine which NICM patients get ICD.
Full text: doi.org/10.1093/ehjc...
#CMR @SCMR #cardiosky
07.10.2025 23:02 — 👍 1 🔁 0 💬 1 📌 0