Aspergillus by @glaucomflecken.bsky.social
19.08.2025 05:43 — 👍 2 🔁 0 💬 0 📌 0
@alukmd.bsky.social
Transplant Infectious Disease physician at Tulane via NYU ID and SUNY Downstate IM. #IDSky #TxID
Aspergillus by @glaucomflecken.bsky.social
19.08.2025 05:43 — 👍 2 🔁 0 💬 0 📌 0
For the awake and dedicated. 7am session - top papers in transplant ID. #TxID #WTC2025
05.08.2025 14:04 — 👍 6 🔁 0 💬 0 📌 0
Don't miss the new @amjtransplant.bsky.social #TxID blog led by Emily Blumberg ajt-transplant-id-exchange.squarespace.com #wtc2025 @ast-idcop.bsky.social @ast-tyfcop.bsky.social @astinfo.bsky.social
03.08.2025 20:01 — 👍 13 🔁 6 💬 0 📌 0
Dr. Robert (Bob) Rubin Transplant ID Award Recipient for 2025 is the amazing @kottonnelson.bsky.social !!! #TxID #MedEd @astinfo.bsky.social
04.08.2025 18:35 — 👍 29 🔁 8 💬 0 📌 1
Packed house at talk on #MDR challenging cases at #WTC2025 - clearly a growing concern in #TxID #IDSky discussion of ceftaz avi plus aztreonam v cefidericol for CRE @ast-idcop.bsky.social @txidfellows.bsky.social @astinfo.bsky.social @ttsorg.bsky.social
03.08.2025 15:36 — 👍 15 🔁 4 💬 0 📌 0
Accuracy of plasma cell-free DNA PCR for non-invasive diagnosis of mucormycosis
@jordan1990.bsky.social and colleagues at Stanford
journals.asm.org/doi/10.1128/...

Lack of Association Between Histoplasma Urine Antigen Values and Clinical Response in Persons without HIV
Marisa Miceli and colleagues
academic.oup.com/ofid/advance...
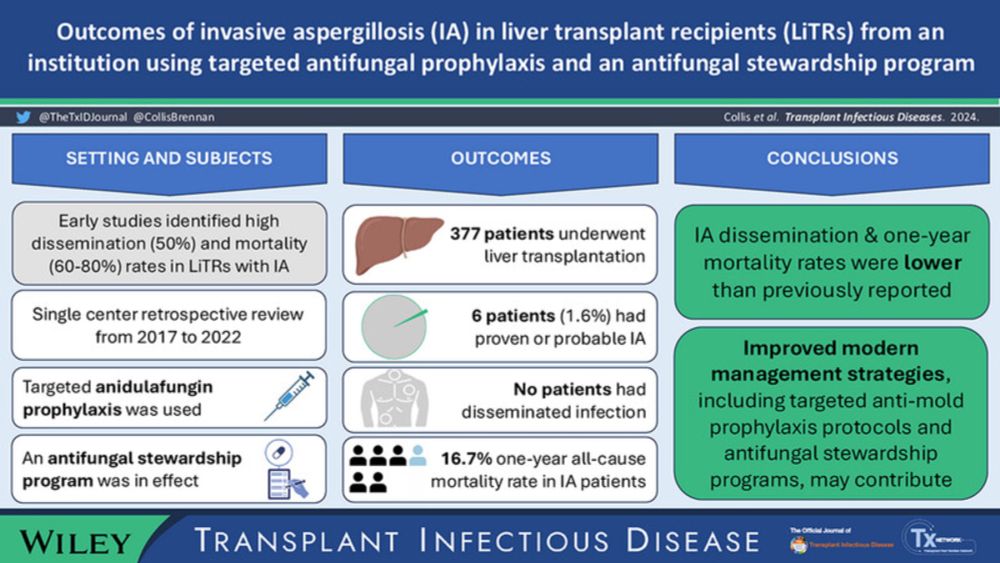
Outcomes of Invasive Aspergillosis in Liver Transplant Recipients From an Institution Using Targeted Antifungal Prophylaxis and an Antifungal Stewardship Program
Duke TxID fellow Brennan Collis and co from Melbourne
IA was uncommon, mortality low in LiTx
onlinelibrary.wiley.com/doi/10.1111/...
Register @ cmvstream.com
23.04.2025 13:34 — 👍 1 🔁 0 💬 0 📌 0
Registration link: cmvstream.com
23.04.2025 13:34 — 👍 1 🔁 0 💬 0 📌 0
🍄🍄Happy to share the link to free full text version of our new article in press: Current Antifungals and the Developing Pipeline with the fantastic @moorewjustin.bsky.social. #IDSky #PharmSky Thank you to the editors @drluiso.bsky.social @alukmd.bsky.social & Dr. Helen Boucher for the opportunity.
24.03.2025 15:18 — 👍 11 🔁 7 💬 1 📌 0
Update on the Clinical Practice Guidelines for treatment of Histoplasmosis. Thank you to all the authors @fungaldoc.bsky.social @germhuntermd.bsky.social @jobadd.bsky.social @iddoc4kids.bsky.social Nathan Bahr
www.idsociety.org/practice-gui...
Facts and myths about measles
@thelancetinfdis.bsky.social @hoferu.bsky.social
www.thelancet.com/journals/lan...

New upcoming seminar from TTS to address a growing concern in the immunocompromised community: Measles
tts.org/116-tts/educ...
😱
06.03.2025 22:13 — 👍 0 🔁 0 💬 0 📌 0Was an honor to work with @drluiso.bsky.social and all the amazing authors who contributed to this issue!
05.03.2025 01:52 — 👍 0 🔁 0 💬 0 📌 0
SCIENCE IN PERIL Research funding at risk UNDERSTANDING RESEARCH COSTS Research requires funding for both direct costs (like lab supplies) and Facilities & Administrative (F&A) costs. F&A covers essential expenses that support research but aren't tied to a single project, such as... IT and cybersecurity for data protection Laboratory space and utilities Administrative support for grants and operations WHAT WILL HAPPEN IF F&A COST REIMBURSEMENT RATES ARE CUT? Research institutions will lose millions of dollars to do critical research THE IMPACTS WOULD BE DEVASTATING. Fewer clinical trials, delaying new treatments Slowed scientific discovery and innovation Weakened local economies and research-driven industries Job cuts and fewer opportunities to train future leaders

Previous F&A cost reimbursement rates varied by institution. Rates averaged around 28%, but some organizations had negotiated rates over 60%. Costs vary widely, with rates set based on factors like institution size, location, and rent or utility costs. HOW IS RESEARCH AT RISK? The National Institutes of Health (NIH) announced a policy change that limits F&A cost funding to 15% for both new and existing grants. The policy drastically cuts essential federal support for biomedical research. A group of universities and states filed a lawsuit claiming the funding cuts are illegal. A federal judge temporarily paused the funding cuts, but F&A costs remain at risk. Scientists and the public are speaking out to share how important it is to maintain funding for research and innovation. RESEARCH SAVES LIVES. NOW, WE MUST SAVE RESEARCH
What’s at stake with proposed health research funding cuts?
Good explainer by Lizzy Knippler, Community Engagement Coordinator at the Duke CFAR. Please share these graphics widely!
The link doesn’t seem to be working?
09.02.2025 01:07 — 👍 1 🔁 0 💬 0 📌 0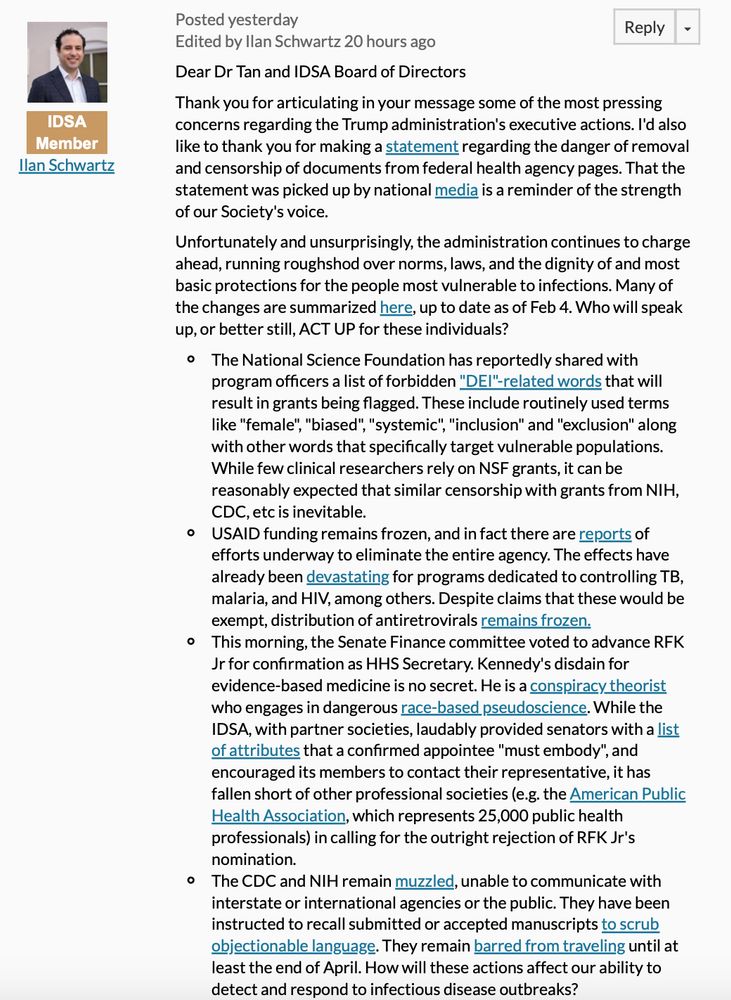
Unfortunately and unsurprisingly, the administration continues to charge ahead, running roughshod over norms, laws, and the dignity of and most basic protections for the people most vulnerable to infections. Many of the changes are summarized here, up to date as of Feb 4. Who will speak up, or better still, ACT UP for these individuals? The National Science Foundation has reportedly shared with program officers a list of forbidden "DEI"-related words that will result in grants being flagged. These include routinely used terms like "female", "biased", "systemic", "inclusion" and "exclusion" along with other words that specifically target vulnerable populations. While few clinical researchers rely on NSF grants, it can be reasonably expected that similar censorship with grants from NIH, CDC, etc is inevitable. USAID funding remains frozen, and in fact there are reports of efforts underway to eliminate the entire agency. The effects have already been devastating for programs dedicated to controlling TB, malaria, and HIV, among others. Despite claims that these would be exempt, distribution of antiretrovirals remains frozen. The Senate Finance committee advanced RFK Jr for confirmation as HHS Secretary. Kennedy's disdain for evidence-based medicine is no secret. He is a conspiracy theorist who engages in dangerous race-based pseudoscience. The IDSA has fallen short of other professional societies (e.g. the American Public Health Association, which represents 25,000 public health professionals) in calling for the outright rejection of RFK Jr's nomination. The CDC and NIH remain muzzled, unable to communicate with interstate or international agencies or the public. They have been instructed to recall submitted or accepted manuscripts to scrub objectionable language. They remain barred from traveling until at least the end of April. How will these actions affect our ability to detect and respond to infectious disease outbreaks?
Meanwhile, our members are experiencing significant moral injury, and some have expressed levels of morale that rival the nadirs felt during the worst of COVID19. Every day it is a new insult, the cumulative effect being the disassembly of public health protections and further marginalization of the most vulnerable in society. Reticence to call attention to ourselves, potentially putting our work in the administration's cross hairs, is entirely understandable. After all, we don't want to imperil existing and ongoing advocacy efforts, including those related to bolstering the ID workforce. A sober analysis would concede that the likelihood of any potential actions moving the needle on any of these issues is low. I would argue, however, that standing up for what is right is the most important thing we can do to reinforce our commitment to social justice and to our members and the patients in our care. What we can do and how we can do it is up for debate; some bold ideas have already been presented in the IDea exchange forum and I welcome further input from colleagues. What is certain is that as rank-and-file individuals, our voices can easily be dismissed, but as a trusted, bipartisan professional organization that represents >13,000 infectious diseases experts, we cannot be ignored, and we must not allow ourselves to cower in silence. The reality is that things are going to get worse, and standing up to the assault on public health will only get more difficult as the administration becomes further emboldened and the actions set in motion gather steam. In the words of John Lewis, "If not us, then who? If not now, then when?"
I am deeply disappointed by the subdued response of the Infectious Diseases Society of America (@idsainfo.bsky.social) to the dismantling of public health structures, both in the US & globally
Here's what I wrote in the closed listserv (response: 🦗) in hopes of stimulating discussion here #IDSky

Visual Abstract
Would global warming bring an increase of invertebrate-associated cutaneous invasive fungal infections?
Kontoyiannis & Casadevall
journals.asm.org/doi/10.1128/...
Congratulations 🎉
29.01.2025 22:08 — 👍 0 🔁 0 💬 0 📌 0
Great work by CDC (Mycotic Diseases Branch) and @grthompsonmd.bsky.social. Healthcare data analysis evaluating fluc efficacy on pulmonary #coccidioidomycosis in immunocompetent patients. Again, fluc is not effective.
#IDSky #MedMyco

The ACIP 2025 vaccine schedule for adults by medical condition (as well as age) is now available - with some great updates www.cdc.gov/vaccines/hcp...
02.12.2024 03:13 — 👍 15 🔁 9 💬 0 📌 0
Figure 1. Study flow diagram.

Figure 2. Patients with proven or probable invasive pulmonary Aspergillus by diagnosis methods.
Evaluation of Viracor Fungal Plus PCR Profile I @MSKCC
"In our cohort, PCR targeting Mucorales and Nocardia can improve the early detection of invasive pulmonary infection, whereas Aspergillus PCR has a low added value"
@fungalspore.bsky.social @ebabady.bsky.social
journals.asm.org/doi/10.1128/...
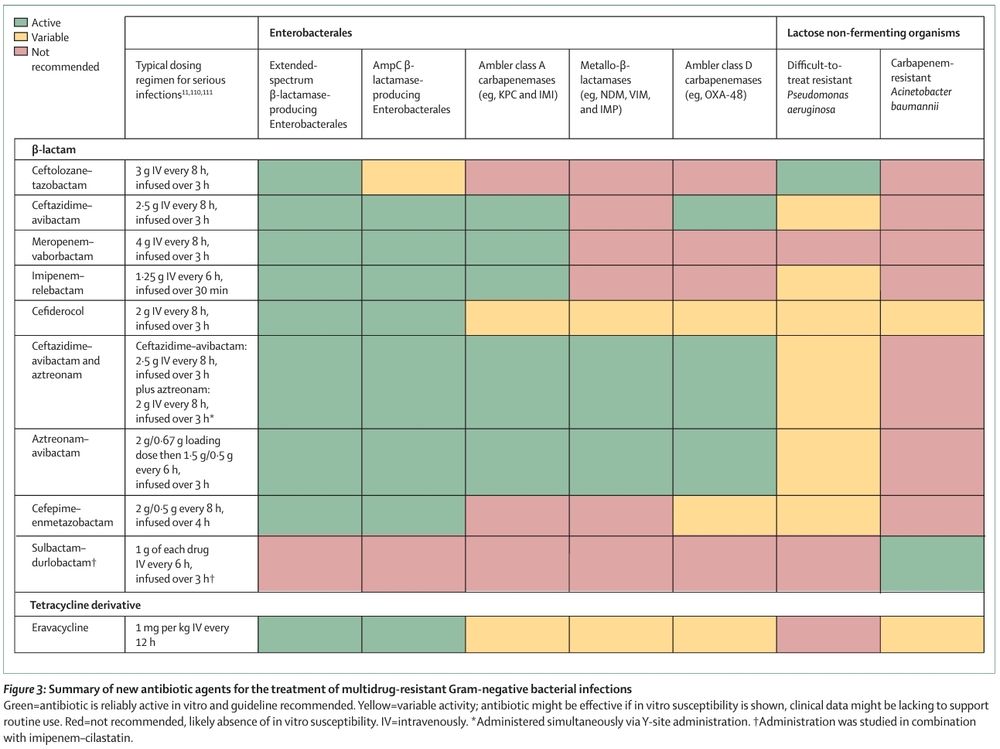
Summary of new antibiotic agents for the treatment of MDR Gram negative bacterial infections
doi.org/10.1016/S014...
#IDSky

Mortality risk according to antiretroviral therapy (ART) status at the time of presentation with cryptococcal meningitis. The dynamic relationship between time on ART at cryptococcal meningitis presentation and mortality risk in the combined Ambisome Therapy Induction Optimisation (AMBITION) and Antifungal Combinations for Treatment of Cryptococcal Meningitis in Africa (ACTA) cohort was determined using univariable logistic regression models with days on ART as the single predictor (using restricted cubic splines with 3 knots) and mortality as the outcome for (A) 2-week and (B) 10-week mortality, restricted to participants on ART for up to 6 months. The gray shading represents 95% confidence intervals. Mortality risk in those on ART for more than 6 months and those not on ART at the time of cryptococcal meningitis diagnosis are shown for comparison, with error bars representing 95% confidence intervals, and the dotted line indicating the mortality risk estimate in those not on ART.
We know that in ART-naive patients with Cryptococcal meningitis, ART initiation should be delayed, but what about those already on ART?
In this retrospective analysis, higher mortality observed w recent ART (<2 wks), and with ART continuation vs interruption
academic.oup.com/cid/advance-...

#idboardreview Pt pricked his thumb w/ wood splinter. 1 wk later, painless papule at injury site & over next weeks, tender lymphangitis developed. No improvement w/oral cephalexin or amox-clavulanate. No fever nor systemic sx, no travel/water exposure #IDSky #idmeded #meded #dermsky
16.01.2025 01:41 — 👍 15 🔁 2 💬 1 📌 0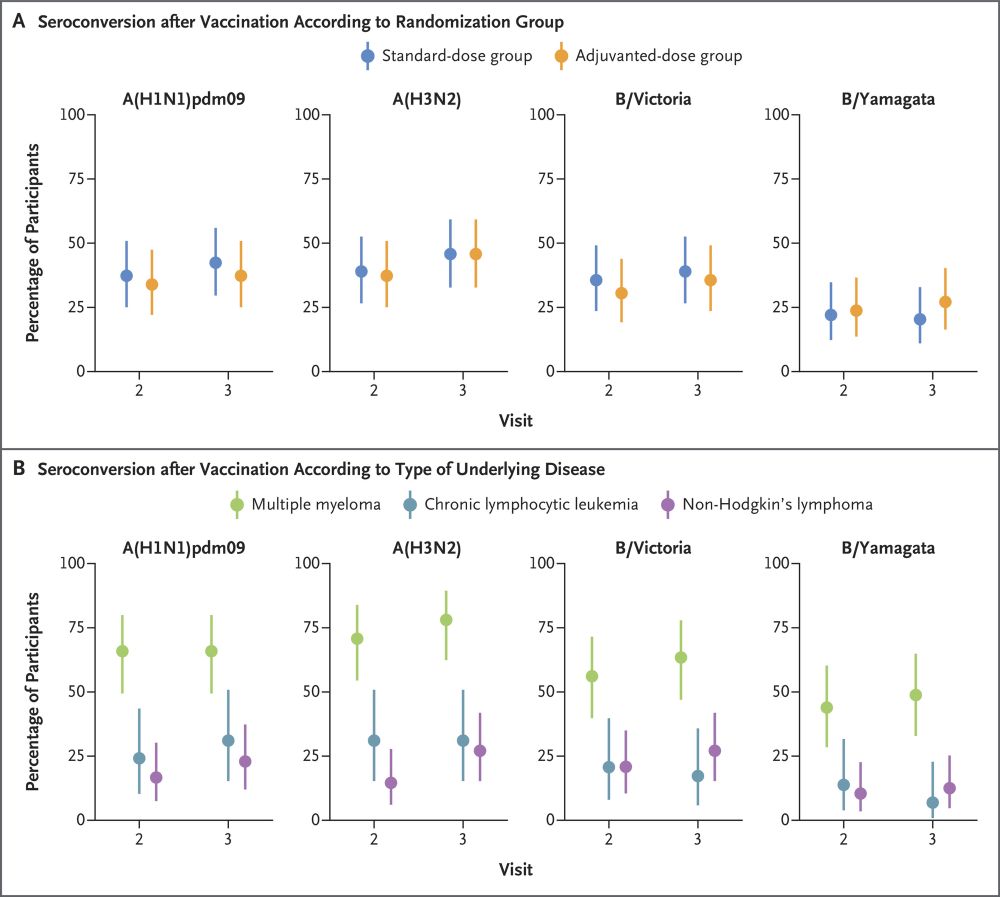
Practice affirming results from our team @victoriahall.bsky.social @ncicancer.bsky.social - No additional benefit from second influenza vaccine dose/adjuvant vaccines in non-HCT haematology patients. #TxID #IDsky #medsky
www.nejm.org/doi/full/10....

Pie charts of whether mold isolates were represented in Bruker and VITEK databases, respectively
Evaluation of two MALDI-TOF MS systems and extraction methods for identification of filamentous fungi recovered from clinical specimens
Eric Ransom, Carey-Ann Burnham and colleagues
journals.asm.org/doi/10.1128/...