


Proposal for an individualized treatment approach in patients with IgA nephropathy (IgAN) ca. 2024
#Nephpearls #NephSky
📌 Hematuria ~ active inflammation 🔥
👉 pubmed.ncbi.nlm.nih.gov/37772889/
Proposal for an individualized treatment approach in patients with IgA nephropathy (IgAN) ca. 2024
#Nephpearls #NephSky
📌 Hematuria ~ active inflammation 🔥
👉 pubmed.ncbi.nlm.nih.gov/37772889/

Treatment of patients with #IgAnephropathy: a call for a new paradigm
doi.org/10.1016/j.kint.2025.01.014
#OpenAccess #NephSky #MedSky #SkyNeph #IgAN #KIReview #kidneydisease
1/ March 28, 2025 - Research Roundtable: The Acid Test - a Patient-led Study of Lactate in ME/CFS and Long COVID
Todd Davenport, PhD, and Ciara Wright, PhD.
A patient-led study, called The Acid Test", formed on Twitter based on reports of abnormal lactate in ME/CFS and Long COVID.

Join us on Tuesday, January 28 at 2 PM ET for "Understanding Genetic Testing Results: Case-Based Illustrations."
Explore the role of genetic testing in CKD, with insights on APOL1, prognosis, and family planning. Earn 1.0 CME credit!
Register: kdigo.co/Module-3-Genetic-Testing-CKD-Webinar-Reg
The excellent overview of IgA management and the upcoming @kdigo.org guidelines from Prof IgA himself, Dr Barratt
youtu.be/OChs5BcTEGE?...
#NephGR #NephSky
Congratulations! So lovely to see you pop up on my feed with such fantastic news x
10.12.2024 09:21 — 👍 1 🔁 0 💬 1 📌 0
Thought should leave this here
journals.physiology.org/doi/full/10....
Randomised to get 5-10mg dapagliflozin. Can't see in abstract or press releases how the dose was assigned. Any idea @hswapnil.bsky.social @jamiekwillows.bsky.social
26.11.2024 21:17 — 👍 0 🔁 0 💬 0 📌 0@jamiekwillows.bsky.social I was looking through the UKKA guidelines (18 oct 21) for this but couldn't find it. Just seen its in the 2023 update! But not that summary figure. Where is that one?
26.11.2024 20:51 — 👍 2 🔁 0 💬 1 📌 0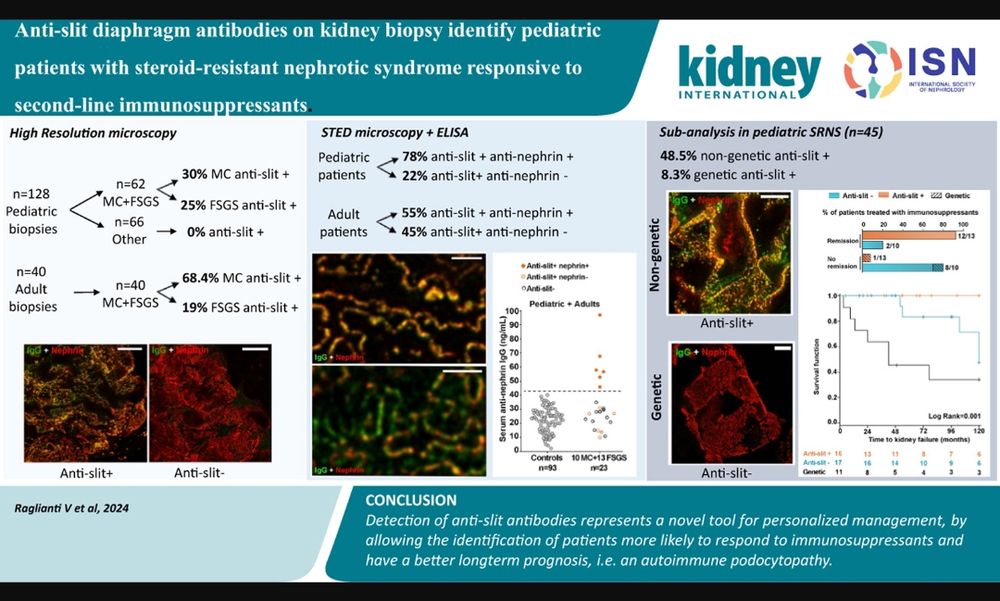
🆕 Antibody identified in podocytopathies 🫘after Anti nephrin Ab⭐
Anti Slit diaphragm Ab ‼️‼️‼️
The heterogeneity in response to immunosuppression is understandable now!
#Nephsky
CAR-T therapy. Again in trials currently
24.11.2024 11:33 — 👍 3 🔁 0 💬 1 📌 0Perhaps we could design investigations template for ME/CFS patients with polyuria....this should be part of standard care so should not be classified as research. First step would be detailed fluid balance chart to understand patterns. Alongside autonomic diary if pts well enough. Focus group?
23.11.2024 21:42 — 👍 0 🔁 0 💬 0 📌 0@dr-kevinlee.com And endocrinologists!
23.11.2024 21:33 — 👍 0 🔁 0 💬 0 📌 0
Its v complicated! Yes but hypoK not all renal wasting. Managed to ⬇️ that. Redistribution in setting of hypovolaemia & high lactate.
Renal tubular and mitochondrial genetic screen negative. Working diagnosis ME/CFS with secondary tubular dysfunction
pmc.ncbi.nlm.nih.gov/articles/PMC....
#NephSky more on mechanisms of polyuria in ME/CFS. Hypovolaemic dehydration triggering polydipsia. Dysfunction of RAAS system. Really is need for nephrologists to help unpick pathophysiology & manage multi system disease. Any one else have interest?
23.11.2024 21:20 — 👍 5 🔁 0 💬 1 📌 0
One of my sickest patients with ME was labelled with psychogenic polydipsia and denied IV saline. Patrick Ussher explains ‘this myth of psychogenic polydipsia’ in this excellent podcast by my colleague Julie Taylor. He also has a free downloadable book (see below).
www.buzzsprout.com/1939141/epis...
It takes time though and does need services with MDT input..... trying to understand an individuals physiology for purposes of supportive management should not stop once have diagnosis. Similarly to understanding phenotypes of PoTS to direct therapy - it adds to conservative and self management too
23.11.2024 21:03 — 👍 2 🔁 0 💬 0 📌 0How can it be acceptable for hospitals to say no. Need to have guideline of what tests are helpful, how to interpret & what treatment to offer. You can understand why someone who is polyuric may struggle with orthostatic intolerance,⬇️cerebral perfusion etc. Once have angle to work up....
23.11.2024 21:03 — 👍 2 🔁 0 💬 2 📌 0Would be really interesting to study this subgroup. Its so hard since doesn't fit neat box and when issues in multiple pathways hard to work out. Once you start doing Ix can pick apart. And then target. Seeing whether common patterns would be v interesting. We really do need specialist centres
23.11.2024 20:40 — 👍 2 🔁 0 💬 1 📌 0Have you managed to do paired serum & urine osmolarities and electrolytes?
23.11.2024 20:24 — 👍 1 🔁 0 💬 1 📌 0So awful most these pts are not investigated or taken seriously. Really needs early intervention since seems to develop into vicious cycle. Need to try & maintain hydrated state to manage symptoms which is v difficult in the face of a renal concentrating defect. How many of your pts are polyuric?
23.11.2024 20:24 — 👍 1 🔁 0 💬 1 📌 0Renal physiology so complicated at the best of times! Polyuria of any cause can cause loss of gradient in the kidney (medullary washout) with reduced response to ADH. Reports of reduced production too. Found few papers suggesting lactate may cause direct tubular injury.
23.11.2024 20:24 — 👍 1 🔁 0 💬 1 📌 0
I've found this article very helpful before and can see it is also about Patrick.
www.healthrising.org/blog/2023/12...
Hope was resetting gradient step would help and can then maintain K and may recover. Chronic low K can also downregulate aquaporins. Similarities to lithium.
pmc.ncbi.nlm.nih.gov/articles/PMC...
iv fluids actually reduce urine output....
23.11.2024 12:30 — 👍 0 🔁 0 💬 0 📌 0Yes - all options make me nervous. Planning to explore more desmopressin next. Its the polyuria driving the hypok. Acidosis high anion gap driven by lactate. Lot of redistribution with fluids shifts.
23.11.2024 12:25 — 👍 2 🔁 0 💬 2 📌 0Thank you! Urine prostaglandins are actually elevated. Will add to the list of potential options. Looks promising. Both k and HC03 low but correct with iv hydration. So hopefully wouldn't be issue.
23.11.2024 12:15 — 👍 1 🔁 0 💬 1 📌 0suspect this is primary issue and clear picture PEM/PESE. SFN clinically. But tubular dysfunction ➡️ polyuria ➡️medullary washout ➡️ vicious cycle. Hoping if can reset the medullary washout prior management strategies will hold.
23.11.2024 09:20 — 👍 0 🔁 0 💬 0 📌 0Thanks. Remembered your prior post when was considering this approach. Don't want to induce diuresis though! Need to get my head around the physiology.
23.11.2024 08:47 — 👍 1 🔁 0 💬 1 📌 0nephroptosis excluded
23.11.2024 08:38 — 👍 0 🔁 0 💬 0 📌 0