

UKKA BP in dialysis visual abstract
Very practical UK Kidney Association guidelines for management of BP in Dialysis
www.kireports.org/article/S246...
KI Reports
UKKA BP in dialysis visual abstract
Very practical UK Kidney Association guidelines for management of BP in Dialysis
www.kireports.org/article/S246...
KI Reports

Stone prevention algorithm for most and Ca stones

Stone prevention algorithm for uric acid and cystine

Stone prevention algorithm for most and Ca stones
Australian guidelines on stone prevention in KI Reports
www.kireports.org/article/S246...
What do you think @weddelite.bsky.social?

Kimberley resident David Lawford had to wait in Perth until someone in his hometown died before he could get access to dialysis on his return.
14.02.2026 00:38 — 👍 5 🔁 5 💬 0 📌 0This is every transplant physician’s nightmare right now.
08.02.2026 21:38 — 👍 8 🔁 3 💬 0 📌 1@sstoneman.bsky.social fantastic tables - what a resource 📖
06.02.2026 04:57 — 👍 1 🔁 0 💬 0 📌 0
To the Editor: As physicians, we took an oath to care for others and to do no harm, promising, in part, “I will remember that I remain a member of society, with special obligations to all my fellow human beings.” The mandate primum non nocere — first, do no harm — has been ingrained in us since medical school. So here we stand, compelled to share our stories in this moment, so the rest of the country knows what is happening in our state. We are bearing witness to what fear can do to the health of a community. Regardless of whether we have lived here our whole lives or moved here from the other side of the world, we all call the beautiful state of Minnesota our home. We live in big cities, in suburbs, and in rural areas. We work in large health systems, in private practices, at academic health centers, in the VA Health Care System, in federally qualified health centers, and with the Indian Health Service. We care for patients throughout our state from birth to death. We teach the next generation of physicians. In a powerful article in the Journal last spring, Drs. Alice T. Chen and Vivek H. Murthy called on physicians to use their voices to advocate for the health of patients and communities during dangerous times.1 In Minnesota, we have found ourselves in an extraordinarily dangerous time. As the presence here of Immigration and Customs Enforcement (ICE) has increased, our clinic schedules have filled with missed appointments. Patient volumes have plummeted in our emergency departments (EDs). Each of these missing patients represents a lost opportunity: a chance to intervene, to make a diagnosis, to start or alter treatment, or to turn the tide of chronic illness. These aren’t patients who don’t care. These are patients who are terrified. When we call to check on them, they tell us they are scared to leave their homes. Scared to drive. Scared to take a bus. Scared that a walk across a parking lot to clinic — a place meant to heal — could put them and their families …

We also know the mental health impact of this crisis. Political unrest and the unfair targeting of immigrant communities have deepened fear, grief, and division, and we see the emotional toll every day. Patients are presenting with symptoms of post-traumatic stress disorder, with suicide attempts. We sit with people whose loved ones have been detained, families fractured, and communities shaken by uncertainty and loss. Our hearts break for all of them. These are not abstract issues in a news cycle — they are human lives, families, and communities hurting in very real ways. Holding space for this pain has reminded us that suffering affects us all. Fear, grief, and exhaustion cross political and cultural lines. We are not immune simply because we are physicians. Dread, desperation, and isolation tighten their grip day by day. We are devastated to witness a beloved nurse colleague, Alex Pretti, gunned down by federal agents. Some of us step out of our homes to provide care for the people of Minnesota knowing that today might be the day when the amount of melanin in our skin outweighs the degrees we have earned and the people we have healed. And yet we push forward, doing what we can. We make calls to patients, attempting to manage what we can from afar. But too often the calls go unanswered. Are our patients afraid to pick up? Or are they unable? We make covert home visits, organize emergency hotlines. We deliver medications, food, and diapers to those who cannot safely leave their homes. When patients do come to see us, we ensure that they leave with enough medication to (we hope) survive this crisis. We are trained to respond to emergencies. We are trained to go above and beyond in moments of crisis. Whether that means working longer hours tending to the sick or linking arms with vulnerable colleagues to walk them to their cars, we help however we can. Nevertheless, we struggle against feelings of helplessness, especially when we are not allowed to help. We read the …
The @nejm.org publishes this from the Minnesota Physicians Voices
www.nejm.org/doi/full/10....

New out today:
Antiproteinuric Effect of Sparsentan in Patients with Genetic-Associated FSGS Enrolled in the DUPLEX Trial
Genetic FSGS CAN be treated. journals.lww.com/cjasn/abstra...

a conservative dialysis strategy in possibly recovering AKI helps people recover faster!
jamanetwork.com/journals/jam...
in @jama.com from #KidneyWk
Like STARRT-AKi et al, at the other end? Small trial - needs replication or this is common sense?

We are 2 for 2 with positive trials so far. LIBERATE-D shows benefit with a conservative vs conventional dialysis strategy in AKI-D. The difference in mortality is concerning though? Simultaneous pub 👇🏾 #kidneywk
jamanetwork.com/journals/jam...

Nature Reviews Nephrology comment on the harms of NIH grant terminations related to kidney disease
www.nature.com/articles/s41...

⚠️Trial exclusions of pregnant & child-bearing age women🤰an ongoing challenge
🙏 Dr Vesna Garovic highlighting this #KidneyWk @asnkidney.bsky.social

JAMA Clinical Guidelines Synopsis: Classification and Risk Assessment of Chronic Kidney Disease. Guideline Title: KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease.
The KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease recommends using equations that include both creatinine and cystatin C for more accurate GFR estimation and risk assessment in CKD.
ja.ma/43QS5vy

I like to lump patients with type IV collagen variants into 4 main categories that can help predict risk of progression and recommended treatment. #KidneyWk
06.11.2025 18:39 — 👍 6 🔁 4 💬 1 📌 0

Fantastic Day 1 ✅ #KidneyWk @asnkidney.bsky.social
05.11.2025 23:36 — 👍 2 🔁 1 💬 0 📌 0
watch out - ORIGIN-3 and FINEONE
likely simultaneous publications tomorrow morning!
#KidneyWk

Ben Wooden kicks off the #KidneyWk Glomerular Disease conference showing the explosion of discovery of glomerular disease genes since 1990. pubmed.ncbi.nlm.nih.gov/32205319/
05.11.2025 14:13 — 👍 8 🔁 2 💬 1 📌 0
Time for my first ASN 👩🏫 @asnkidney.bsky.social
04.11.2025 20:21 — 👍 6 🔁 0 💬 0 📌 0
A review revealed which #CKD drugs are safe to use while #breastfeeding but evidence for many therapies is still lacking. #kidneydisease #nephrology #nephsky docwirenews.com/post/review-...
19.09.2025 19:03 — 👍 4 🔁 1 💬 0 📌 0
Going to add this to my lecture slides.
26.08.2025 18:05 — 👍 29 🔁 15 💬 0 📌 0
GLP1ra in ADPKD?
pubmed.ncbi.nlm.nih.gov/40815122/

T1b
BP Measurement: In 2017 ‘proper’ technique was recommended and that has transitioned to standardized technique in 2025. Let’s all use a checklist…and let’s use it every time! How close is your regular practice to this standard?
#NephJC

Use of genetics for kidney disease research reveals an array of variants in COL4A genes and a resulting range of disease presentations. From hematuria to Alport syndrome, genetic data has provided a new basic research basis for genotype-phenotype correlations. kidney.pub/KN1707-08 #ASNKidneyNews

Cartoon
Poignant cartoon on therapeutics (here vaccines) in pregnancy
absolutelymaybe.plos.org/2025/06/27/d...
Renalism is a similar issue!
From @hildabast.bsky.social

Cystatin C vs. Creatinine in AKI recovery
eGFRcr may overestimate kidney function post-AKI due to muscle loss. A KI Reports study found eGFRcys was lower, flagged more CKD, and a higher creatinine–cystatin C index (CMI) predicted lower 5-year mortality. www.kireports.org/article/S246...

Promising!
flozination in ADPKD (mostly older adults with DM or CVD) - presumably those with another valid indication - associated with slower GFR slope
journals.lww.com/cjasn/pages/... in @asnpublications.bsky.social #CJASN
With no obvious harm signal

We’re making measles great again
😡😡😡
Hey #NephSky and #MedSky
Check out the VA for our discussion 4/15/25 at 9pm EST
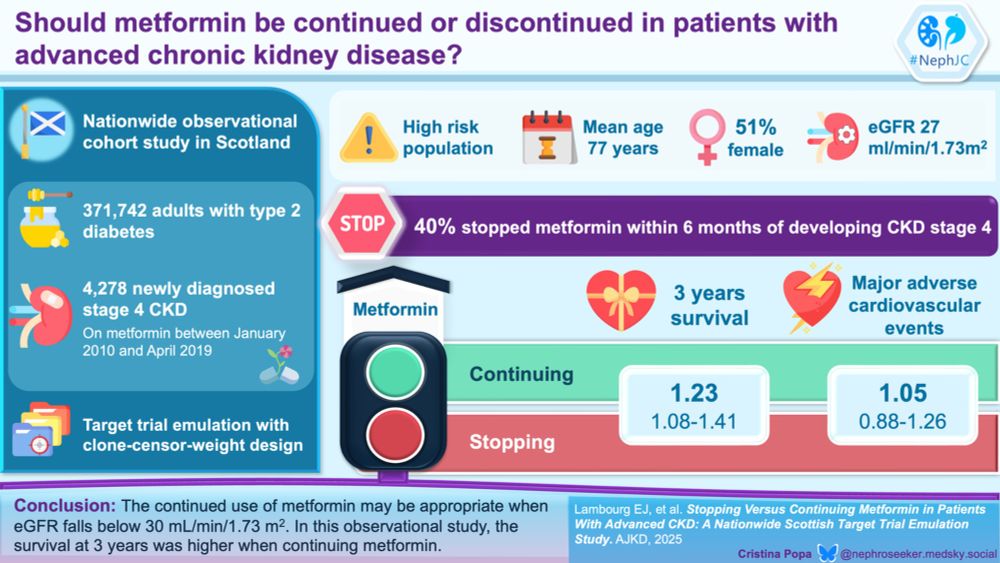
Metformin-Should I Stay or Should I Go (in patients with advanced CKD)
VA by @nephroseeker.medsky.social
www.nephjc.com/news/metformin-ckd-va
Interesting study of sleep duration by using Fitbit trackers in hemodialysis
From the Renal Research Institute in @asnpublications.bsky.social K360
journals.lww.com/kidney360/pa...
1/
#NephSky

Spring has sprung - Vancouver
06.04.2025 17:47 — 👍 2 🔁 0 💬 0 📌 0



Venous Thromboembolism Prevention in Nephrotic Syndrome: The Role of Aspirin, Vitamin K Antagonists, and Direct Oral Anticoagulants ca. 2025 from @kireports.bsky.social @saynanorouzi.bsky.social @kdjhaveri.bsky.social
#Nephpearls #NephSky
👉 www.kireports.org/article/S246...