

va
steroid reduction in GN
www.kireports.org/article/S246...
excellent review by ottawa GN group in @kireports.bsky.social @michael-toal.bsky.social and team
va
steroid reduction in GN
www.kireports.org/article/S246...
excellent review by ottawa GN group in @kireports.bsky.social @michael-toal.bsky.social and team

(A) Diffuse medium and small renal arterial stenoses (yellow arrows) and microaneurysms (red arrows). (B) Intact large abdominal vessel angiogram and a small splenic artery aneurysm (red arrow in inset). (C). Distended arteriole occluded by a thrombus (arrowhead), consistent with thrombotic microangiopathy (PAS stain, ×200).
#Quiz from October 2025:
A 16-year-old male patient presented to an ED with a 3-week history of progressive headaches, nausea, vomiting, and bilateral blurry vision. Over the past 3 days, he developed chest pain and shortness of breath.
bit.ly/47iQnEo

A Man with Asymptomatic Hypertension Sarah Gorey, M.B. You are the intern on call for the night shift. You are paged to come to the surgical ward to assess a patient. A 63-year-old man with uncomplicated diverticulitis was admitted earlier in the day for antimicrobial and conservative treatment. He rarely visits his family doctor, is not aware of having high blood pressure, and does not take regular medications. You have been called because on a routine check of vital signs, the patient’s blood pressure was 185/115 mm Hg. All other vital signs were within normal limits. The patient has no symptoms; he has no headache, dyspnea, or chest or abdominal pain. He reports feeling slightly stressed at being admitted to the hospital today, which he was not anticipating, but had been sleeping comfortably before the nurse checked his vital signs. On examination, he appears to be comfortable, and there is no clinical evidence of withdrawal from alcohol or other substances. His abdomen is soft and nontender, and on auscultation, no bruits are heard over the aorta or renal arteries. His pulses are 2+ and symmetric in all anatomical distributions. You note that his blood pressure was also high (166/97 mm Hg) at admission 4 hours earlier and had not been measured again until now. Routine laboratory test results from blood samples obtained at the time of admission show increased levels of leukocytes and inflammatory markers but normal kidney and liver profiles. The nurse manager confirms that the blood-pressure monitors on this ward have been calibrated recently. A repeat blood-pressure measurement obtained after the patient has rested quietly for 10 minutes is still elevated, at 182/103 mm Hg. You must decide whether the patient’s blood pressure should be monitored over time on an outpatient basis (a “watchful waiting” approach) or whether he should begin receiving antihypertensive medications during this hospitalization.
Should we be treating inpatient hypertension?
Interesting case with two discussants (Michael Rothberg vs Tara Chang)
www.nejm.org/doi/full/10....
I have to confess despite being a nihilist for treating inpatient BP I am tempted to do something in this setting.

The December 2025 issue is available now: bit.ly/43SrjDd
Highlights:
- Intronic and Coding Genetic Variants in Autosomal Recessive Polycystic Kidney Disease Among Israeli Bedouins of Arabian Peninsula Ancestry
- Nephrologist Perspectives on Using Telemedicine During In-Center Hemodialysis

T0j: #NephJC
The ORIGIN phase 2b trial
👥 116 patients with biopsy-proven IgAN and persistent proteinuria despite RASi
💉 Weekly atacicept 150 mg (wk 36)
⬆️ 35% greater UPCR reduction vs placebo
⚙️ a mean eGFR benefit of +5.8 mL/min/1.73 m²
pubmed.ncbi.nlm.nih....

T0f: #NephJC
1️⃣In IgAN, mucosal dendritic cells activate Tfh cells and directly drive B‑cell class switching via BAFF and APRIL, generating pathogenic IgA ☠️
2️⃣The expansion and mis‑trafficking of Gd‑IgA1+ B cells 👉 excess circulating Gd‑IgA1
pubmed.ncbi.nlm.nih....
T0c: #NephJC
First, the guideline seems outdated. Until now, we aimed to slow CKD progression 🐌, but what if we look from a more daring perspective? Like oncologists/ rheum…
With armamentarium we have now, we can aim for remission 🛑, dare I say “cure”?
pubmed.ncbi.nlm.nih....
Thank you 🙏
19.11.2025 02:11 — 👍 1 🔁 0 💬 0 📌 0
✍️Check the insightful #NephJC summary by @notjustdialysis.bsky.social
19.11.2025 02:04 — 👍 6 🔁 3 💬 1 📌 0
Arshad Ali, Michigan
No COI
love this topic
#NephJC

Mouse Alport podocytes are susceptible to AAV9 transduction in vivo
doi.org/10.1016/j.kint.2025.09.027
#MedSky #NephSky
@jeffminerphd.bsky.social @washunephrology.bsky.social @washumedicine.bsky.social

EDITORIAL by Pascale Khairallah, Elizabeth Lorenz, and Puneet Sood:
Rethinking Transplant Care Through a Sex- and Gender-Based Lens
bit.ly/433XPly (FREE)



Freely Filtered dives into ACHIEVE with Mike Walsh. This was a great episode. Also with show notes, chapters, and key images (if your podcast client supports it) www.nephjc.com/freelyfilter...
02.11.2025 14:01 — 👍 14 🔁 7 💬 2 📌 0
💗 Loved this episode. The puns were great, the trial story is even better! What really stood out was the resilience behind it.
✨Five tries to ACHIEVE the first grant, then 11 in total

T0c
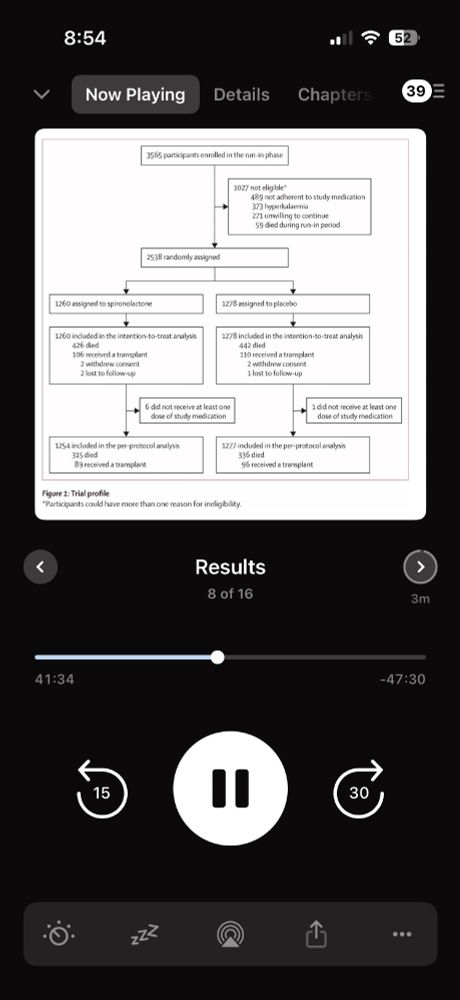
There have been numerous developments in the field of transplantation that have improved outcomes and success rates. Today 95% of renal transplants are functional after 1 year, and 80% at five years. #NephJC
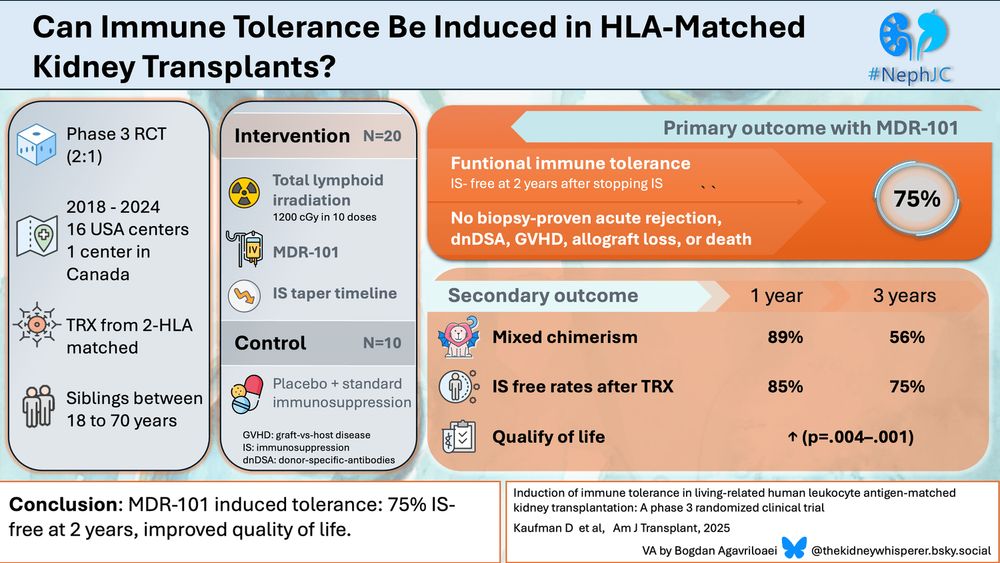
🎨Beautiful visual abstract by
Bogdan Agavriloaei @thekidneywhisperer.bsky.social #NephJC
Arshad Ali, Michigan
No COI
#NephJC
Reminder that primary hyperparathyroidism can be a cause of hypertension!
25.07.2025 13:03 — 👍 11 🔁 2 💬 1 📌 0
Urine CXCL-9, now in immune checkpoint inhibitor AIN! In @kidneyint.bsky.social
www.kidney-international.org/article/S008...
Her serum creatinine has been around 0.7 all along. Over last 2-3 years she had noticed a trend going up and was referred to evaluate. Genetic testing we orderly routinely for this subset of patients who have no known etiology. Agree at this time we would just not do anything.
18.06.2025 03:02 — 👍 2 🔁 0 💬 0 📌 0
Agree!
She had no problematic pregnancies.
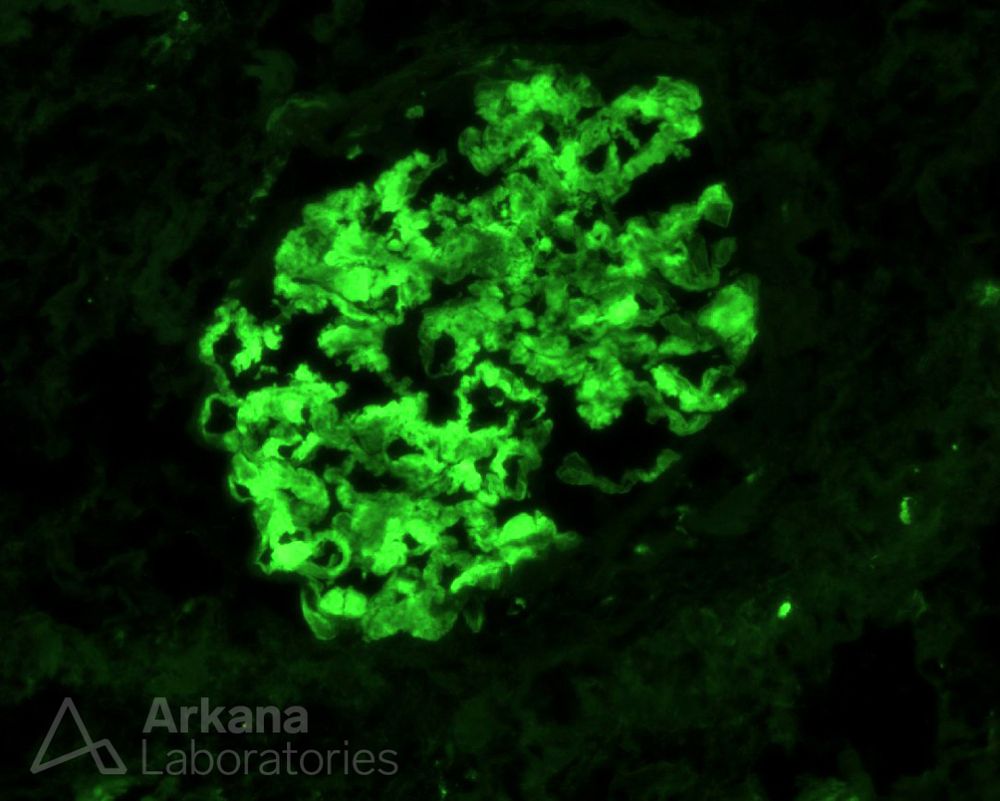
What is your leading diagnosis when seeing this interesting IgG staining pattern by IF?
#DiagnoseThis #pathology #renal #kidneypath

Triple drug combo now available in US - approved by FDA
Telmisartan 10
Amlodipine 1.25
Indapamide 0.625
george-medicines.com/george-medic...
#Hypertension
#Widaplik
Also in higher doses:
20/2.5/1.25 and
40/5/2.5

Machine Perfusion in Deceased Donor Kidney Transplantation: Editorial Summary of a Cochrane Review by @samjtingle.bsky.social and Colin Hugh Wilson
bit.ly/AJKD25Tingle... (FREE)
Serology including ANA , C3C4 ANCA are all normal.
No other signs or symptoms.
Other than actual measuring Factor H levels and vaccinations and treating infections, is there any role for Eculizumab in such patients.
@askrenal.bsky.social
How do you manage a 70 yr old female with stable renal function with serum creatinine at 1.12 with positive heterozygous CFH complement factor H deficiency on genetic testing with urine sediment showing oval fat bodies with no proteinuria or hematuria. UPCR/ UACR negative.

Suzetrigine: Is It A Safer Pain Medication For Patients With Kidney Disease?
www.renalfellow.org/2025/05/02/s...

Cool diagnosis in a dialysis patient
www.nytimes.com/2025/05/02/w...
@rmcentor.bsky.social in the NYT
H/t @doctorajgu.medsky.social
#NephSky
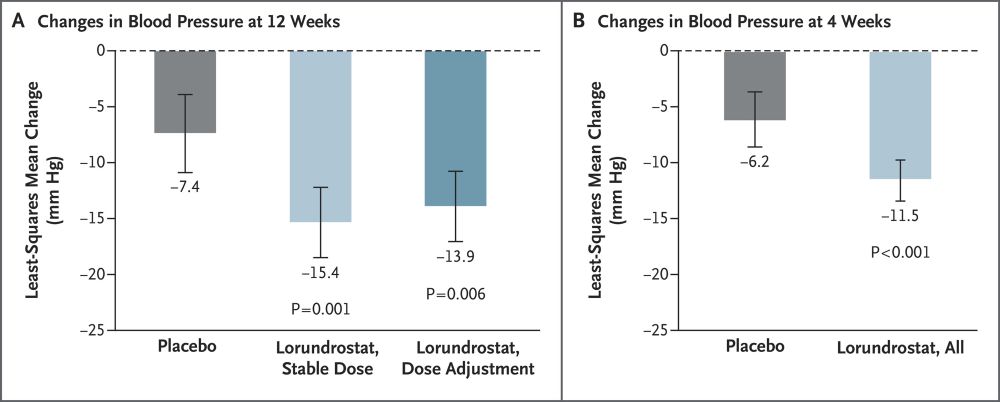
The ASIs have arrived
www.nejm.org/doi/full/10....
Aldosterone synthase inhibitors - first one to finish the phase 3 line
#Lorundrostat #Hypertension
