Yes, always
22.10.2025 01:27 —
👍 1
🔁 0
💬 1
📌 0
#tumorboardtuesday
🤔Hmmm....much more rapid disease progression on the CDK4/6🚫+AI - does this portend for a worse prognosis in subsequent lines of therapy❓
22.10.2025 00:48 —
👍 1
🔁 1
💬 0
📌 0
7/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 4🏫
💊Several FDA👍PIK3CA-inhibitors: Capivasertib or Alpelisib or Inalvosalib
🤔 When and how do you PIK one of the PIK3CA of the 3 available?
☝️Inavolisib+Fulvestrant+Palbo is approved for 1st line mER+ BC after recurrence on/after adjuvant ET therapy
22.10.2025 00:38 —
👍 3
🔁 1
💬 1
📌 0
7/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 4🏫
💊Several FDA👍PIK3CA-inhibitors: Capivasertib or Alpelisib or Inalvosalib
🤔 When and how do you PIK one of the PIK3CA of the 3 available?
✌️Alpelisib & Capivasertib are approved in 2nd line mER+ BC combined with fulvestrant
🔎 NGS results, Baseline A1C
22.10.2025 00:38 —
👍 2
🔁 1
💬 1
📌 0
8/18 #TumorBoardTuesday
Back to our case🔎
👩🦳 Patient received Capivasertib + Fulvestrant due to PIK3CA mutation.
👉 Not yet considered endocrine resistant so would not move onto capecitabine, sacituzumab
👉 Tumor is HER2 negative so no role for trastuzumab deruxtecan
22.10.2025 00:38 —
👍 1
🔁 1
💬 1
📌 0
8/18 #TumorBoardTuesday
Back to our case🔎
👉 Everolimus + fulvestrant is not favored given the more targeted approach with Capivasterib for the PIK3CA mutation
✅ Tolerated therapy well with mild rash at start of treatment that resolved with antihistamines
22.10.2025 00:38 —
👍 1
🔁 1
💬 1
📌 0
9/18 #TumorBoardTuesday
⏭️ Case 2
#TumorBoardTuesday #OncTwitter Case 2
👩🦳 62 y.o. postmenopausal female
💉 mBC to the🫁, ER 70%, PR 85%, HER2⛔[IHC 1] 🩻 confirmed⬆️Dz on 1L ribo/letrozole at C7
🏃♀️ ECOG PS 1. No co-morbidities.
⛔ Normal vital signs, labs
🩸Liquid Biopsy shows ESR1 mutation, TMB-High
22.10.2025 00:40 —
👍 1
🔁 1
💬 2
📌 0
10/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 5🏫
👉 Recurred on adjuvant endocrine tx
👉 Recurred <2y after adjuvant endocrine tx
👉 ⬆️Dz<6mos of starting 1L mBC tx
👉 ⬆️Dz after any duration of >=2nd line of ET-based therapy
👉 Known ESR1 mutation [now have 2 Rx for ESR1m → elacestrant or imlunestrant]
22.10.2025 00:42 —
👍 1
🔁 1
💬 1
📌 0
11/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 6🏫
EMERALD
👩🦳 2L metastatic HR+/HER2- received 💊 Elacestrant, an oral selective ER Degrader (SERD)
✅ 1-2 prior ET including CDK4/6i and < 1 chemo
💊 Elacestrant 400mg daily vs 💉fulvestrant or 💊AI
⬆️⬆️ PFS for prior💊 CDK4/6i > 12 mon with ESR1 mutated tumors
22.10.2025 00:45 —
👍 1
🔁 1
💬 1
📌 0
ASCO Publications
11/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 6🏫
⬆️ Elacestrant benefited all subgroups including: 🦴only, 🫁 visceral mets, > 3 mets
⬆️ Elacestrant benefited all🧬subgroups: ✔️ESR1+PIK3CA, ✔️ESR1+TP53, ✔️ESR1+HER2-low
🤢 Most common AE: N/V
22.10.2025 00:45 —
👍 1
🔁 1
💬 1
📌 0
#tumorboardtuesday
Any subtle differences in outcomes based on the specific mutation identified
AKT vs. PTEN vs. PIK3CA❓
22.10.2025 00:29 —
👍 1
🔁 1
💬 0
📌 0
3/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 2🏫
CAPItello-291
👩🦳 mER+/HER2- breast cancer with PD on AI +/- CDK4/6i
💉2L Fulvestrant +/- capivasertib [oral, 🚫AKT plus.. 🚫PTEN, 🚫PIK3CA]
...continued
22.10.2025 00:21 —
👍 1
🔁 1
💬 1
📌 0
4/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 3🏫
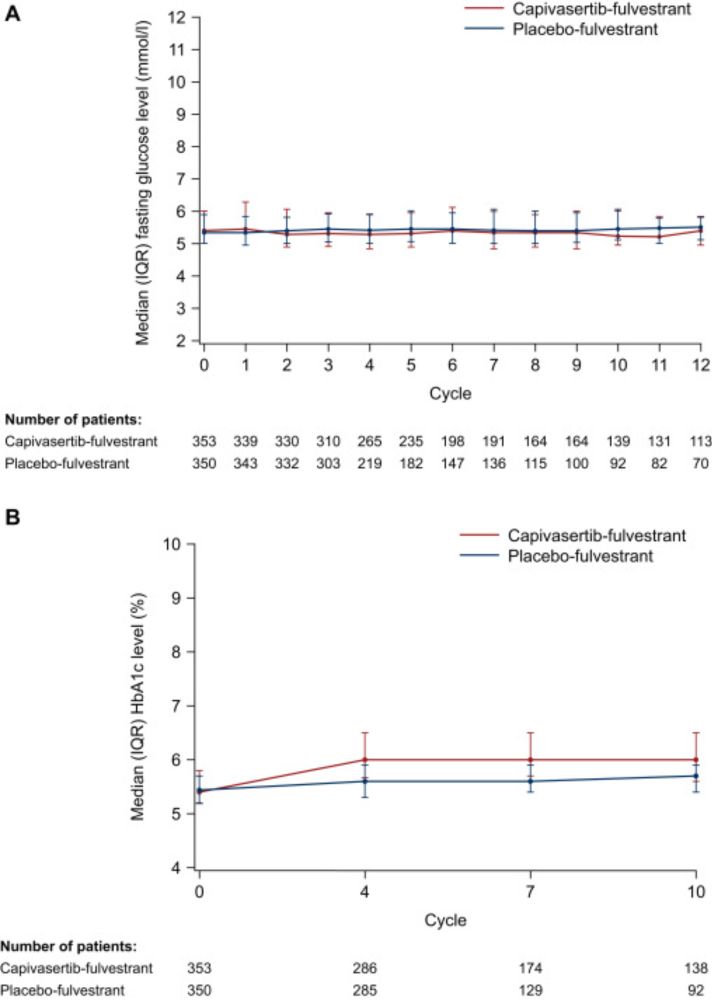
CAPItello-291: Capivasertib Side effects
💊 Capivasertib taken 4 days on, 3 days off per week
🩺 Need baseline A1C < 8%
🚽 Most common AE: Diarrhea onset ~ day 8 [All grades 72%, G3/4 9.3%]
...continued
22.10.2025 00:23 —
👍 1
🔁 1
💬 1
📌 0
5/18 #TumorBoardTuesday
Back to our case🔎
💉 57yo ♀️ with mBC to the 🦴, liver, ER 100%, PR 95%, HER2⛔[IHC 0]-🩻confirmed⬆️Dz on 1L ribo/letrozole at C47
✅ Normal labs (A1C=5.8) & VS
🩸Liquid Biopsy: +PIK3CA mutation, TP53 mutation, TMB-Low (4 mut/mb), High tumor fraction (> 5%)
👩🏻⚕️What 2L Tx is advised❓
22.10.2025 00:25 —
👍 1
🔁 1
💬 1
📌 0
6/18 #TumorBoardTuesday
POLL
What 2L therapy would you give this patient❓
1) Capecitabine
2) Trastuzumab deruxtecan
3) Sacituzumab govetican
4) Capivasertib + Fulvestrant
5) Everolimus + Fulvestrant
22.10.2025 00:26 —
👍 1
🔁 1
💬 1
📌 0
2/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 1🏫
...cont
📝Tissue-based assays or plasma-based assays (ctDNA) can be used
☝️Some alterations may be better detected by tissue-based assays like homozygous loss of PTEN or TMB-H.
☝️Liquid assays may reflect tumor heterogeneity more accurately
22.10.2025 00:15 —
👍 2
🔁 1
💬 1
📌 0
2/18 #TumorBoardTuesday
👩🏻🏫Mini Tweetorial 1🏫
Actionable Mutations in 2L mER+/HER2- BC
🧬Several actionable mutations in 2L+ mBC: ESR1, PIK3CA, AKT, PTEN, BRCA (germline, somatic)
🔍Evaluation of acquired mutations at progression will help to direct therapy options
Cont.....
22.10.2025 00:15 —
👍 1
🔁 1
💬 1
📌 0
#TumorBoardTuesday POLL
What would you do next❓
1) Start capecitabine
2) Liquid biopsy to assess for actionable mutations
3) Start trastuzumab deruxtecan
4) Check tumor markers Ca 15-3 & Ca 27.29
22.10.2025 00:07 —
👍 1
🔁 1
💬 1
📌 0
1/18 #TumorBoardTuesday
@KennaKoehler & @drgattimays.bsky.social
Case 1
👩🦳57 y.o. postmenopausal female
📋Well controlled DM (A1C = 5.8)
🏃♀️ECOG PS 0
💉Metastatic BC to bones, liver, ER 100%, PR 95%, HER2- [IHC 0] w/scan confirmed progression on 1L ribociclib/letrozole at C47 in bones
⛔ Normal labs & VS
22.10.2025 00:03 —
👍 1
🔁 1
💬 1
📌 0
#TumorBoardTuesday
📢Join us Tuesday, 10-21-25 at 8PM ET as @drgattimays.bsky.social &
@KennaKoehler 🗣️ Tx options after CDK4/6⛔️: What to consider in the 2nd line for HR+/HER2– mBC❓
RT and bring others into the discussion‼️
21.10.2025 12:39 —
👍 1
🔁 1
💬 1
📌 0

#TumorBoardTuesday
🧠And while we finalize the case details, collect FREE #CME
👉🏽https://integrityce.com/tbt2025
21.10.2025 12:39 —
👍 1
🔁 1
💬 1
📌 0
#TumorBoardTuesday
➡️Before @drgattimays.bsky.social & @KennaKoehler 🗣️ 2nd line Tx options for HR+/HER2– mBC, #BCSM tell us your connection to this medical🩺discussion
👇👇🏼👇🏾
1) Onc/Surg/Rad/IR/Gyn Onc
2) Other MD/APP/RN/Pharm D
3) Patient/Patient Advocate
4) Fellow/Resident/Trainee
21.10.2025 12:39 —
👍 1
🔁 1
💬 1
📌 0
✅This #TumorBoardTuesday🗣️with @KennaKoehler & @drgattimays.bsky.social is provided by @IntegrityCE
👍Supported by ed grants from Exelixis, Ferring, Ipsen, Lilly, Janssen Scientific Affairs, Merck & Taiho Oncology 🙏
👉🏽Info about 🆓 CME: integrityce.com/tbt2025
21.10.2025 12:39 —
👍 1
🔁 1
💬 1
📌 0
#PreTest Q1️⃣#TumorBoardTuesday Free #CME integrityce.com/tbt2025
B4 @KennaKoehler & @drgattimays.bsky.social🗣️2nd-line Txs for #breastcancer, test your🧠with these 2❓
21.10.2025 12:39 —
👍 1
🔁 1
💬 1
📌 0
🤔What 2L Tx would you offer a 45yo♀️w/ AKT mutated, ER+/HER2- mBC after⬆️Dz on ribociclib➕AI/OFS❓
1) Capecitabine monotherapy
2) Capivasertib+fulvestrant
3) Elacestrant monotherapy
4) Everolimus + fulvestrant
21.10.2025 12:39 —
👍 1
🔁 1
💬 1
📌 0
#PreTest Q2⃣#TumorBoardTuesday
🧐 A 75yo♀️w/ER+/HER2- PIK3CA+ mBC is starting 2L therapy with alpelisib+fulvestrant. Baseline A1C=6.1 & BMI is 33. What steps can limit risk for severe hyperglycemia❓
1) Labs QW x 2, then monthly
2) Baseline A1C, then q3 mos
3) Consider metformin
4) All of the above
21.10.2025 12:39 —
👍 1
🔁 1
💬 1
📌 0