

It’s been a while, #MedSky
Been busy with a top-priority project 🥰
It’s been a while, #MedSky
Been busy with a top-priority project 🥰
Fabulous little thread on #LungUltrasoung
Agree with all of these! 🙌
#emimcc
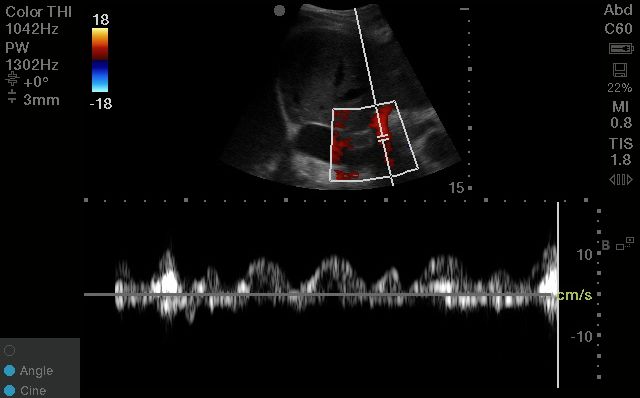
Fair, but we’re looking at patterns of pulsatility, not measured amplitude; I think the former would be preserved
26.02.2025 20:53 — 👍 1 🔁 0 💬 0 📌 0Not really, as long as you’ve got a segment aligned vertically on your screen (ie you don’t want to be seeing a short-axis cut of it)
25.02.2025 20:42 — 👍 2 🔁 0 💬 1 📌 0
So: want to learn more about portal venous doppler and #VEXUS?
Dr Curro Mirrales is speaking all about Portal Venous waveforms at #HR25 - come learn from the best!! May 22-23 in Montreal 🇨🇦. Grab your spot today!!!
ccusinstitute.wixsite.com/ccus/events/...

Likewise, their IVCs and hepatic veins (because of the proximity to the IVC) will always be abnormal.
By moving farther away to the portal vein, we can get a better reflection of organ congestion with diuresis, as was elegantly demonstrated in this recent paper
pubmed.ncbi.nlm.nih.gov/38734970/
3. It's the most useful in those challenging patients with severe TR
The R-heart failure/severe TR patients are often the most challenging to assess in terms of congestion.
Many of them will ALWAYS live at a high CVP.
2. It's the easiest to interpret
Unlike the hepatic vein, which can be misleading in the absence of EKG gating, the portal vein is easily interpreted
You can use calipers to measure pulsatility fraction; but you can also use the eyeball method to assess mild vs moderate vs severe pulsatility.
You should see a nice vertically-aligned segment of the portal vein pop into view; easily recognized by its bright hyperechoic borders and hepatopetal blood flow (which will look RED on colour doppler).
25.02.2025 18:30 — 👍 3 🔁 0 💬 1 📌 0
1. It's easy to obtain
Unlike the intra-renal veins, which can be elusive even to the most experienced scanners, the portal vein is usually easily identifiable.
From R coronal plane in the mid-axillary line, with your liver/kidney in view, fan or slide your probe in the anterior-posterior plane.
A quick #VEXUS thread 🧵-
3 reasons why the portal vein is the most useful single venous doppler waveform 🥇
(if you're only going to do ONE site to look for venous congestion, this is probably the most useful one!)
#emimcc
Whether you work in a ward setting, critical care unit, or emergency department - I guarantee you will learn something from him!
Come join us at #HR25! May 22-23, 2025 🇨🇦
ccusinstitute.wixsite.com/ccus/events/...
In the wise words of @drfreeze.bsky.social - "The goal is to titrate PEEP to the triad of best compliance, best oxygenation, and best RV function" 🫁🫀👍
An intensivist, physiology enthusiast, and all-star medical educator, he'll be speaking at #HR25 all about next-level Non-Invasive Ventilation ✨
Non-invasive positive pressure ventilation - BiPAP and CPAP, for example - can be a bit of a black box to most of us ⬛️
Once it's started, the nuances of how to adjust it to optimize each patient's physiology takes skill, experience, and often, a bit of trial and error 🔎
#emimcc
Yeah definitely lots of local variation; and ICU carries its own set of needs due to the extremely high acuity. I think many of these are fairly universal though!
16.02.2025 16:27 — 👍 1 🔁 0 💬 1 📌 0I love that question - “can anyone think of anything we’re missing?” Medicine is a team sport and I value feedback from everyone!
14.02.2025 17:03 — 👍 5 🔁 1 💬 0 📌 0
There is lots more to be said here, so I'm curious to hear from others: what are your top tips for efficient rounding? 👩⚕️📋⏰💉🤓
#MedSky #skeetorial #emimcc #InternalMedicine
Especially early on in training, I would MUCH rather see trainees who are very thorough in their rounding, even if they take slightly longer; than those who race to finish and miss important details.
14.02.2025 16:32 — 👍 4 🔁 0 💬 1 📌 0
10. For early trainees: don't sacrifice thoroughness for efficiency
All this being said: a huge part of rounding efficiency comes from experience. As you become more comfortable managing common problems and your knowledge base expands, so too will your rounding efficiency 🧠
The patient admitted with pneumonia who had half a second of brief tingling pain in their big toe, now resolved - probably doesn't need an urgent CT scan.
The vasculopath admitted for heart failure who has new colour change and pulselessness in their foot, in contrast, certainly does!
9. Not everything has to be an issue
This comes largely with experience and a growing knowledge base, but knowing when something is an issue that requires further (possibly urgent) investigation, and when something can be safely deferred or observed, is a key skill 🗝️
8. Batch work
This is not always possible for patient care and flow reasons, but I do find it helpful ✅
For example: I will often save my discharge summaries and do these after completing my rounding on all my patients.
But if you can, try to set aside focused work periods and minimize interruptions that are not time-sensitive ⏰
Having a dedicated time to discuss with Allied Health, for example; or a system whereby nurses can leave non-urgent messages for the care team (without a phone call/page), can be helpful
7. Avoid interruptions*
I know, I know - this can be next to impossible in a hospital setting, especially in certain environments. (Hats off to all my EM friends who manage near constant interruptions!)
When I round the next day, I can quickly and easily see my proposed plan.
That's not to say that your plan can't change from day to day, but it makes it much easier if you've already done the initial cognitive legwork.
6. Make life easier for your future self
When I am writing my Assessment/Plan section, I try to think ahead for each issue. What will the next step be? If X happens, what will I do? What about if Y happens? 🤔
You do not have to restate every single investigation since admission. You do not have to rewrite all the information you've included earlier in your note.
Be complete, but be concise: edit your note frequently. State the current issues, DDx for these, and next steps.
5. Less is more
A very common mistake I see trainees make is the ESSAY of a rounding note, especially the Assessment/Plan section (made even worse by the copy/pasting of prior notes).
There is a temptation to include every piece of information in your Assessment/Plan section - resist this! ❌
4. Get to know your EHR
Electronic Health Records are supposed to make our lives easier.
Most have areas of frustration, but becoming facile with the time-saving features of your EHR can really boost your efficiency ⏫
For example: templates for common text, shortcuts to pull in common labs, etc
As much as you can, flesh out your issue and priorities before entering the room, so that you can make sure to ask the key questions and examine your patient appropriately.
This means prepping your note and issues list, and processing the patients results, before stepping in the room.
