
There is always an XKCD
12.01.2026 08:58 — 👍 3648 🔁 815 💬 7 📌 5There is always an XKCD
12.01.2026 08:58 — 👍 3648 🔁 815 💬 7 📌 5Do you have access to Terlipressin in the US? We use it quite a lot, 4 hourly dosing so can usually be given on the ward and sometimes keeps them out of the ICU (when not in MOF..)
06.11.2025 18:52 — 👍 1 🔁 0 💬 1 📌 0
Agree the POCUS pendulum has probs swung a bit too far in some areas.
I think it can be helpful occasionally - i.e. cardiac standstill as a negative prognostic marker in prolonged arrest maybe?
Certainly shouldn’t prolong the pulse check or get in the way of good ALS
LV vent? More of a guess than a confident answer..
26.09.2025 19:37 — 👍 2 🔁 0 💬 1 📌 0
If there are categories, I would add “performative cricoid pressure”, which involves lightly touching the neck without applying any real force as to not distress the patient when we don’t think cricoid is really necessary but are afraid of litigation..
Probably the worst of the three.
Very interesting! All endovascular or did you have to go on circ arrest?
19.07.2025 10:40 — 👍 2 🔁 1 💬 1 📌 0Leiomyosarcoma? Or thrombus?
18.07.2025 18:11 — 👍 1 🔁 0 💬 1 📌 0
The caveat with in-plane is that it’s fairly easy (I find) to accidentally slide off the jugular and onto the carotid if they are side by side.
It does prevent going through the back wall and cannulating a posterior artery though I guess.. no one failsafe technique.

Hard lessons re cardiogenic shock at #SoA25 - refusal of ICU admission because of lack of organ support needs at that point always irks me.
In a sick patient with multi organ dysfunction we clearly ought to intervene early to mitigate the need to organ support - are we too reactive as a specialty?
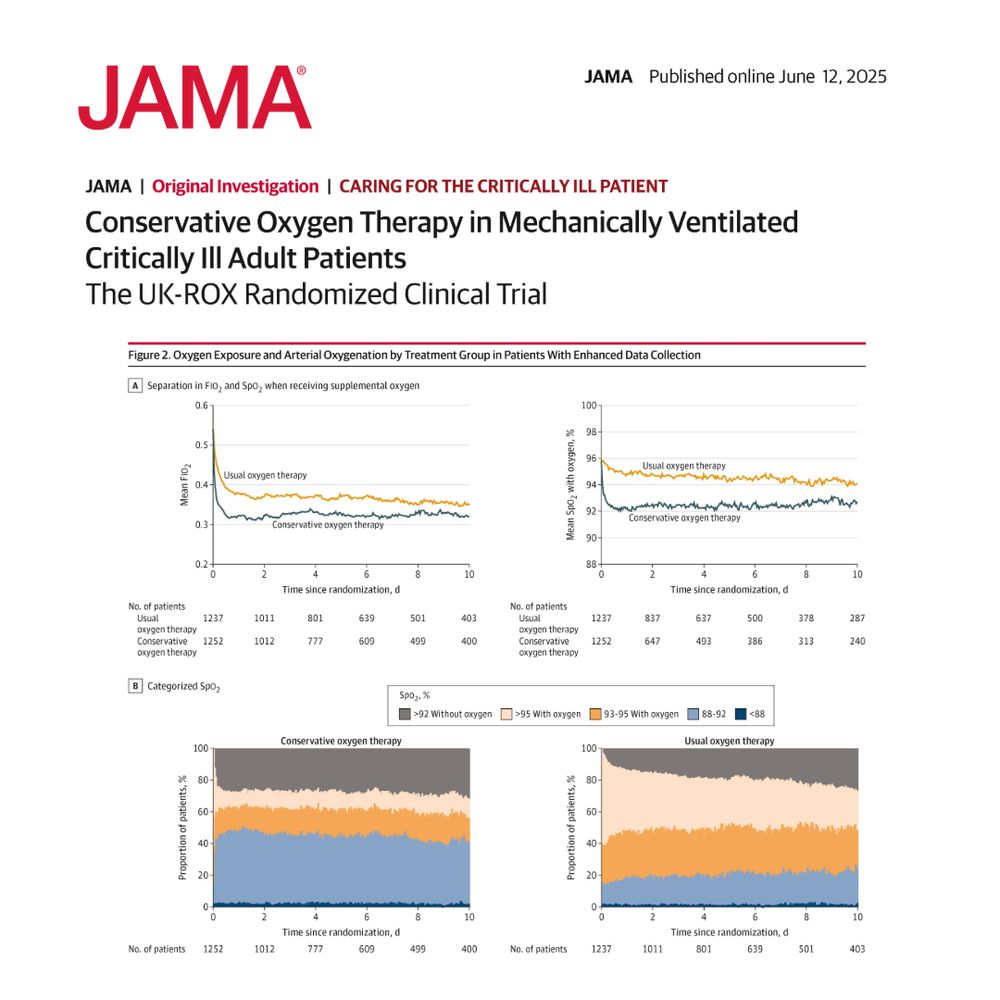
Figure 2. Oxygen Exposure and Arterial Oxygenation by Treatment Group in Patients With Enhanced Data Collection
Conservative oxygen therapy with a target SpO2 of 90% did not reduce 90-day all-cause mortality compared to usual oxygen therapy in mechanically ventilated adult patients.
#CCR25 @criticalcarereviews.com
https://ja.ma/4kG5gWK
Not sure why APRV is such a polarising subject. It does seem to work in some patients (?recruitability), very difficult to get hard data on this.
Would also argue that is has a more favourable adverse effect profile than VV ECMO so why not try?

Donald Trump’s gargantuan self-dealing | Opinion
https://www.ft.com/content/f1cf9453-8fc4-49d5-9781-e117f744c3c7
Everyone should ideally leave twitter and come to bluesky for several reasons.
- Unify the discussion
- Safe space for everyone (eg LGBTQ)
- Stop supporting twitter (which is now a vehicle of misinformation & political manipulation)
- Twitter is currently NSFW (eg frankly pornographic content)
I’d say TIVA for most elective work where smooth offset, less of PONV etc is most important.
Don’t tend to use it for high stakes emergency work (sick laparotomy, big traumas) - worried about giving lots of propofol in those and also reducing anaesthetic complexity lets you focus on resuscitation
Apart from all the reasons you stated, I also think the FICM favours anaesthesia residents, not so much in terms of content but in the way it is delivered (anaesthetists will be used to viva examinations, and the OSCE is very different from PACES)
30.04.2025 12:38 — 👍 3 🔁 1 💬 0 📌 0Interesting argument! Out of interest, what motivated you to sit EDIC as well?
29.04.2025 13:52 — 👍 2 🔁 0 💬 1 📌 0
Interesting as the effusion does not look huge, but presumably acute hence the rapid progression to tamponade?
Would definitely say RA collapse and maybe some RV collapse on diastole when I try to slow it down
Scary what’s going on in the US right now - but also clearly legally highly dubious?
18.04.2025 12:10 — 👍 0 🔁 0 💬 0 📌 0
Time to dump my shares in Sedaconda!
Inhaled Sevoflurane led to increased 90d mortality compared to propofol (52.9% v 44.3%) in pts with ARDS
(Also median duration of NMB use of 5 days in both groups seems wild 🫤)
jamanetwork.com/journals/jam...
#MedSky #EMIMCC
Highly recommended for anyone with even a fleeting interest in cardiothoracic anaesthesia!
10.02.2025 09:11 — 👍 1 🔁 0 💬 0 📌 0
How do you use it on your unit? Only ever used it as infusion on ICU but seen it given as bolus in cardiac anaesthesia for RV dysfunction coming off bypass.
Nebulised conceptually makes sense but never seen this in practice
Agree, our approach of having a different storage layout in almost every theatre is baffling. Should be able to standardise within institutions if not across.
Same with clinical rooms on wards - assembling equipment for a procedure often takes longer than procedure time..
vasopressin challenge: this group evaluated 1U bolus of vasopressin to evaluate patient responsiveness
I love this for a few reasons:
[1] allows vaso to have rapid onset (rather than taking 30-60 min to build up)
[2] we can get a sense of whether the vaso is helping
🧵 1/5 #EMIMCC
Speaking about my own patch… Wales has the lowest number of ICU beds per head of population in the world - and you can’t do that in the community.
These conversations shouldn’t be an either/or between primary and secondary care. It needs to be asking what are hospitals *for*?

The last days of Walter Benjamin
https://www.ft.com/content/fe8d0d96-ccbf-4410-8955-306987aea3b5

Wrote a little piece for the @ficm.bsky.social Resident’s Eye Newsletter on our forays into tabletop simulation on the ICU - have a read!
11.01.2025 18:23 — 👍 4 🔁 0 💬 0 📌 1I would argue that truly difficult intubations where removing the tube would be dangerous are rare - PUMA guidelines provide an algorithm for this, too.
06.01.2025 11:05 — 👍 2 🔁 0 💬 1 📌 0This argument seems to be recurring on a regular basis. Don’t think this is a significant issue - in the vast majority of cases removal & re-intubation is arguably safer than leaving ETT in situ.
06.01.2025 11:05 — 👍 4 🔁 0 💬 2 📌 0