#emergency #emergencymedicine #criticalcare #icu #airway #medic #science #data #research #army #armymedicine #armyemdoc #trauma
30.04.2025 00:43 — 👍 0 🔁 0 💬 0 📌 0
So, either (a) you should be less worried about putting in an IO when you need vascular access, (b) you should rethink your stance on NG tubes, or (c) both.
Clip from The Pitt on @StreamOnMax
www.annemergmed.com/article/S019...
pubmed.ncbi.nlm.nih.gov/10339680/
PMID: 10339680
30.04.2025 00:43 — 👍 3 🔁 1 💬 1 📌 0
To that end, in the same study that assessed NG tube placement, NGT placement was rated by patients as more painful than ABG, abscess I&D, urinary catheter placement, fracture reduction, and lumbar puncture.
30.04.2025 00:43 — 👍 0 🔁 0 💬 1 📌 0
Comparatively, another study used the VAS to assess other common ED procedures. NG tube placement was rated at 46 out of 100mm... so, more painful. Yet, most of us probably do not think twice about ordering NG tubes.
30.04.2025 00:42 — 👍 0 🔁 0 💬 1 📌 0
Are IO's actually that painful to insert? Can they be used in awake patients?
This is over-dramatized. Yes, they can be used in awake patients.
One study assessed the pain associated with humeral IO insertion and removal finding a mean reported pain of 3.9 and 2.2 on a 10-scale, respectively.
30.04.2025 00:42 — 👍 0 🔁 0 💬 1 📌 1
In many cases, elective surgeries that could require blood were delayed until adequate supplies were available.
Clip from The Pitt on Max
pubmed.ncbi.nlm.nih.gov/35729854/
#emergency #emergencymedicine #criticalcare #icu #airway #science #data #research #army #armymedicine #armyemdoc #blood
24.04.2025 01:44 — 👍 0 🔁 0 💬 0 📌 0
This was most pronounced during early COVID when there was not only on-going demand for product (trauma, transplant and cancer never stopped existing), but donations were very scant with schools and business sources for blood drives dried up.
24.04.2025 01:44 — 👍 1 🔁 0 💬 1 📌 0
There is no good data on how often this happens, nor is there a standard threshold. This will often be a discussion between the surgical team, anesthesiologist, and the ICU team with the blood bank. The usual first step is that the blood bank will reach out to their supplier.
24.04.2025 01:43 — 👍 0 🔁 0 💬 1 📌 0
Lessons learned from the COVID-19 pandemic blood supply crisis - PubMed
Lessons learned from the COVID-19 pandemic blood supply crisis
Larger centers are provided more products by the suppliers, which can be affected by things like trauma designation, transplant center status, etc.
24.04.2025 01:42 — 👍 0 🔁 0 💬 1 📌 0
Anecdotally, I was lucky enough to transfer out hemorrhaging patients from critical access facilities before exhaustion occurred. I'm sure others have been less lucky.
24.04.2025 01:41 — 👍 0 🔁 0 💬 1 📌 0
Lessons learned from the COVID-19 pandemic blood supply crisis - PubMed
Lessons learned from the COVID-19 pandemic blood supply crisis
This usually only happens at large, tertiary care centers. Smaller hospitals often have very limited blood supplies on hand, so the response at those hospitals is to transfer the patient to the center with the larger supplies on hand, not bring in more supplies to the small hospital.
24.04.2025 01:41 — 👍 0 🔁 0 💬 1 📌 0
Lessons learned from the COVID-19 pandemic blood supply crisis - PubMed
Lessons learned from the COVID-19 pandemic blood supply crisis
Essentially, it means that the blood bank is either going to run out of supplies or their supplies will become depleted to the point that it risks other patient care activities, usually the latter.
24.04.2025 01:41 — 👍 0 🔁 0 💬 1 📌 0
Can the blood bank run out of blood?
Well, yes, and no. Every hospital has their own thresholds for which they can request additional resources. This is sometimes referred to as a "catastrophic" activation.
24.04.2025 01:39 — 👍 0 🔁 0 💬 1 📌 0


#tbt 2023 versus 2016... Fort Bliss the sign was a lot cooler 😎 back in 2016
#emergency #emergencymedicine #military #army #armyemdoc
20.07.2023 04:45 — 👍 1 🔁 0 💬 0 📌 0
RCT published in Crit Care this week finds no benefit to prone positioning 🛌 in hypoxic COVID-19 patients with regards to:
-Progression to NIV or intubation
-Death
Major limitations:
-Median time prone per day was 90m, goal was 2h
-Only 1/3 of those assigned proning qualified for the per-protocol
19.06.2023 22:38 — 👍 2 🔁 0 💬 0 📌 0
When it comes to airway, there's not too many things worse than an unrecognized tube in the goose.
This systematic review assessed clinical methods when the gold standard waveform ETCO2 is not available:
Misting = 🗑 🗑 (FP=69%)
Auscultation = 🗑 (FP=18%)
Colormetric CO2 = 🤏 (FP=5%)
19.06.2023 21:13 — 👍 1 🔁 0 💬 0 📌 0
Acute subdurals are easy to manage from the ED standpoint.
Chronic subdurals, not so much. It's often something we find incidentally, and they may or may not have symptoms (e.g. fell down, hit head, no symptoms, etc.).
The DESCA trial came out this week, and sheds light on what doesn't work.
19.06.2023 16:03 — 👍 0 🔁 0 💬 0 📌 0

The DHA and 59MDW funded DEVICE trial results are out.
It's clear that video laryngoscopy is superior to direct laryngoscopy.
The military needs to field VL technology to every medical footprint on the battlefield.
Time now.
17.06.2023 20:29 — 👍 2 🔁 0 💬 0 📌 0
The results from our DEVICE trial are out in the @NEJM . In this RCT, direct laryngoscopy was inferior to video laryngoscopy for first-pass success.
In fact, it was so inferior that we had to stop the trial early after DSMB review due to the clear benefit of VL.
16.06.2023 18:07 — 👍 1 🔁 1 💬 0 📌 0
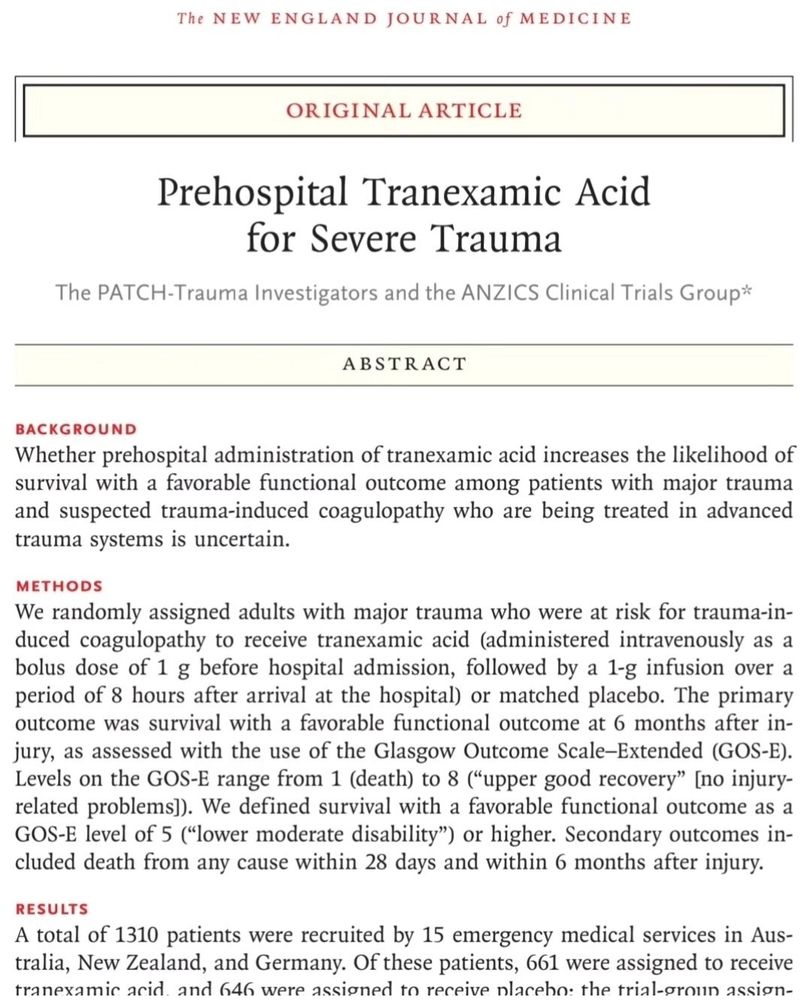
🔥 off the press (hours ago) in @NEJM, the PATCH trial finds no benefit with prehospital TXA at 6 months based on GOSE.
14.06.2023 15:55 — 👍 4 🔁 0 💬 0 📌 0







