Do we REALLY not have time for that? Sometimes “thinking out loud” and concluding in a sentence or two would be more than enough. Would benefit the resident doctors, bedside nurses and whoever is scribing too.
We need not to make education an added extra or afterthought
28.04.2025 10:44 — 👍 1 🔁 1 💬 1 📌 0
Productivity in healthcare is a problematic term because it is hard to define and near impossible to measure, if we accept the premise that quality is at least as important as quantity.
26.03.2025 23:25 — 👍 2 🔁 1 💬 0 📌 0
This is a deeply depressing article. Change and innovation thrive in a culture which gives people the tools they need to do the job & supports positive risk-taking. If your hospital is inefficient because the ceiling is falling in or the IT is ancient, cutting the tariff won't drive improvements.
26.03.2025 12:14 — 👍 50 🔁 20 💬 6 📌 1
We’re keeping the focus on the pressures facing our EDs today. Speaking to Nick Triggle, BBC health correspondent, RCEM President expressed the College’s concerns about the unintended risk related to incentivising ED waiting time targets which may lead to some of the most vulnerable patients waiting
Risk of incentivising ED waiting time targets - RCEM President Dr Adrian Boyle
#ICYMI: In the morning, RCEM expressed concerns about the unintended risks of incentivising ED waiting time targets, highlighting that it might leave some of the most vulnerable patients waiting the longest.
That afternoon, the Health Secretary replied. Watch below.
youtu.be/osz6QaPkLwQ
15.03.2025 10:34 — 👍 9 🔁 6 💬 0 📌 0
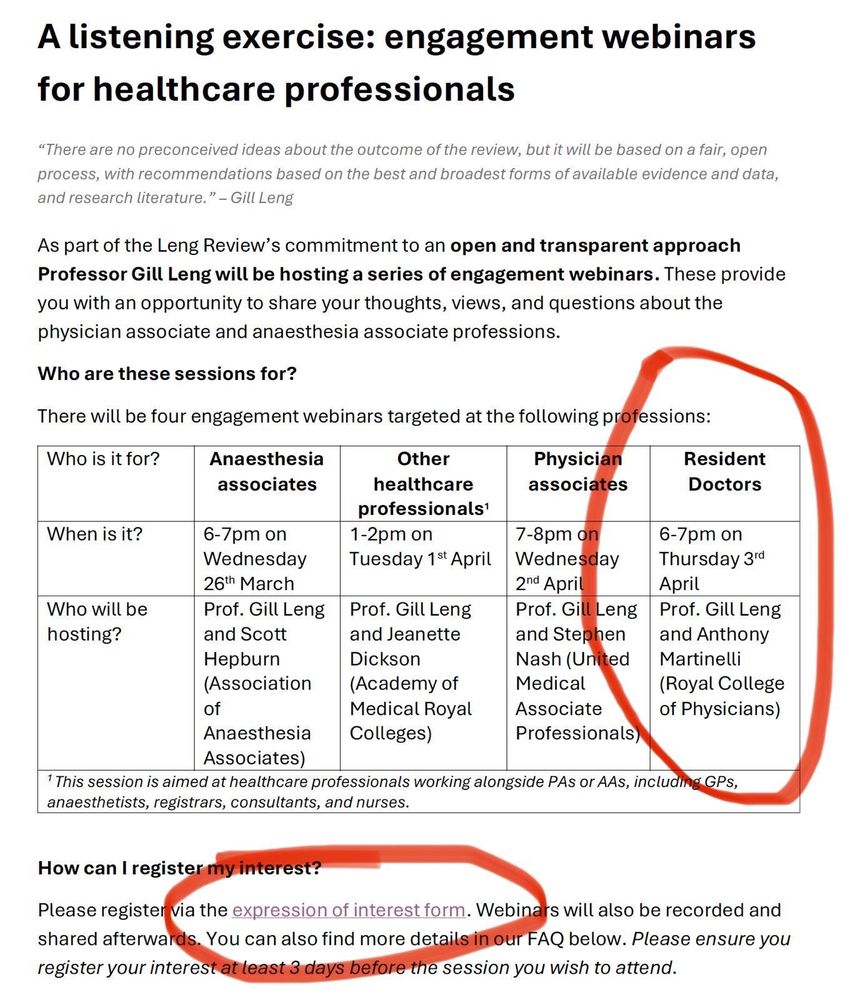
💥 DOCTORS!💥
Please share.
The #LengReview is running 2 engagement webinars for doctors:
🩺 Resident doctors: 6pm, 3 April
🩺 Other doctors: 1pm, 1 April
You can sign up for both here with your NHS email:
forms.office.com/Pages/Respon...
14.03.2025 11:45 — 👍 22 🔁 24 💬 0 📌 3
Remember this is the very small % that have passports and have ever left the boundaries of the USA.
14.03.2025 14:51 — 👍 2 🔁 0 💬 0 📌 0
News to me!
However if I were to guess, I’d suggest that farming out minor injuries provision to private providers (with varying levels of actual minor injury training), and not ensuring EM doctors actually get decent minor injury training, probably hasn’t helped?
13.03.2025 20:10 — 👍 4 🔁 1 💬 1 📌 0
Fundamentally, this document encapsulates deep misunderstanding about Medicine.
We TEACH medical knowledge in a sliced and diced up way, because the subject is vast and one has to arrange knowledge somehow.
The PRACTICE of Medicine is essentially COGNITIVE. How we think
9/
12.03.2025 11:56 — 👍 8 🔁 2 💬 1 📌 0
Define “everything”. Are we proposing crashing them onto ECMO? (Presumably not, though at this point I’m no longer sure!)
Offer everything reasonable that has a realistic chance of success. But these things aren’t realistic or reasonable. Neither is CPR in this population
04.03.2025 17:42 — 👍 0 🔁 0 💬 1 📌 0
Same reason as not offering them a heart transplant or ECMO. It won’t work, it’s a futile brutal burdensome treatment.
04.03.2025 17:33 — 👍 0 🔁 0 💬 0 📌 0
And medically nonsense, but Americans going to American I guess!
04.03.2025 14:26 — 👍 1 🔁 0 💬 1 📌 0
Good reason: patient is 100 years old, frail and underlying cause for death is not reversible (given its old age).
04.03.2025 14:09 — 👍 0 🔁 0 💬 1 📌 0
I think it’s pretty cruel actually for doctors to abnegate responsibility and expect grieving relatives with no medical training or understanding of what CPR can and cannot do, to effectively say “yes let grandma die”.
The framing of the explanation is key. CPR does not work in ordinary dying.
04.03.2025 14:02 — 👍 1 🔁 0 💬 2 📌 0
I would immediately take the family aside and explain that their relative has died and that we would be discontinuing CPR because it was not going to be effective and was denying them peace and dignity at their last moments. This would very much be a (kind & gentle) statement of fact not a question
04.03.2025 13:59 — 👍 1 🔁 0 💬 1 📌 0
The unrealistic portrayal on TV is unhelpful, and the unrealistic expectations of families can be hard to manage. Frank and timely conversations are important.
I’d expect that someone frail should have been given the protection of a DNACPR/RESPECT form while able to discuss
04.03.2025 13:54 — 👍 1 🔁 0 💬 2 📌 0
No I mean the converse, when CPR is appropriately not done.
I’m on board with sueing regarding battery and desecration of a corpse!
04.03.2025 12:48 — 👍 1 🔁 0 💬 1 📌 0
In the UK at least there is no obligation for healthcare professionals to provide futile and inappropriate treatments. In reality, second opinions, long conversations etc.
What if they demanded a heart transplant, or ECMO? Why do we treat CPR differently?
04.03.2025 12:22 — 👍 1 🔁 0 💬 0 📌 0
Sue on the grounds of what exactly? They were never going to survive? How bizarre
04.03.2025 12:20 — 👍 0 🔁 0 💬 2 📌 0
Yep. But how are “middle ground” cases handled? So let’s say an 88 year old with pneumonia and bronchospasm- where IV antibiotics and oxygen maybe appropriate, but say NIV and bronchoscopy may not be.
Or a ‘well’ 104 year old who would like antibiotics for sepsis, but definitely shouldn’t have CPR?
04.03.2025 12:18 — 👍 0 🔁 0 💬 1 📌 0
So this may be part of the US-UK disconnect with this case. UK nursing homes are generally for those with high level nursing care needs (bed bound, dementia, multimorbidity, frailty).
We’d use the term “residential home” for those receiving bed &breakfast and social support
04.03.2025 08:34 — 👍 0 🔁 0 💬 1 📌 0
That’s fairly disgusting and depressing. All the more reason though to embed and discuss ceilings of treatment and DNACPR preemptively.
From this side of the pond it feels like the US has a dichotomy between “do everything” and “hospice” (which seems to be do nothing?) without middle ground?
04.03.2025 08:30 — 👍 2 🔁 0 💬 2 📌 0
Though after a prolonged prehospital low flow period, prognosis is almost certainly dire in a patient like this regardless of all the cleverness and advanced techniques. In which case some kindness, privacy and calm is probably a better management plan.
04.03.2025 00:18 — 👍 4 🔁 0 💬 1 📌 0
I’m not sure there’s enough info on baseline in the original post to determine this (in UK ‘nursing home) implies high care needs/advanced frailty and I’m not sure if this is the same in the US. In advanced frailty all this is clearly inappropriate, futile and undignified.
04.03.2025 00:16 — 👍 6 🔁 0 💬 2 📌 0
In a situation like this where a DNACPR or RESPECT form has unfortunately not been completed, & resus commenced, the receiving team would make an assessment of prognosis and appropriateness of ongoing resus
04.03.2025 00:14 — 👍 5 🔁 0 💬 1 📌 0
In patients who have a low likelihood of meaningful recovery following a cardiac arrest, the ideal scenario is a preemptive discussion with patient and family to explain that “full resus” would not be in the pts best interest for these reasons.
04.03.2025 00:13 — 👍 4 🔁 0 💬 1 📌 0
I tried and was turned down. But have managed it for a resident.
20.02.2025 20:27 — 👍 0 🔁 0 💬 1 📌 0
I am fairly sure that all this may have been in either “improving junior doctors working lives” or “promoting excellence”’both of which say the right kind of things overall. But there’s no teeth in enforcement and that’s what is desperately needed
20.02.2025 20:27 — 👍 0 🔁 0 💬 0 📌 0
I believe people may be working on this. I agree would be a game changer. Can occasionally be managed in special circumstances
20.02.2025 20:24 — 👍 2 🔁 0 💬 1 📌 0
Do Americans DO high school biology? It’s very hard to tell.
20.02.2025 20:21 — 👍 8 🔁 0 💬 4 📌 0
The unofficial account for the Emergency Medicine Research Team at the Royal Oldham Hospital , Greater Manchester UK.
Part of the Northern Care Alliance NHS Trust .
🌤️ Hello, I’m the Mental Elf!
🌳 Follow me to keep up to date with the latest reliable #MentalHealthResearch.
👩🏽💻 #WorldBipolarDay webinar on March 30th
🍄 Do you need some #ElfHelp? https://elfi.sh/help
🔗 https://linktr.ee/thementalelf
Emerg/Stroke/Flight Doc.
Lover of Med Ed, mountains, and neurocritical care. Also a Ninja.
#UCalgary #EMCases #STARSAirAmbulance #SYNAPSECourse
Consultant dermatologist in the UK. Worried about the state of the
NHS. Concerned about the GMC.
Anaesthetic consultant. Dabbles in healthcare policy & healthcare data geek. Feminist & European
Leader of @LibDems.org.uk, husband, father, carer, and MP for Kingston & Surbiton.
Promoted by Liberal Democrats, 66 Buckingham Gate, SW1E 6AU.
Academic HPB Surgery Resident. Pancreas 2000 Scholar. Interested in the pancreas, liver and associated giblets. Views Own.
Welcome to the official Bluesky account for the New England Journal of Medicine. Follow for high-quality, peer-reviewed research and clinical content from the world’s leading medical journal, online at NEJM.org.
Follow @ai.nejm.org for medical AI content.
EM doc, mum of footballers, clarinet tootling.
UK Doctor, aiming for EM. Happiest on a hilltop in shitty weather.
I mainly like listening to heavy music and ascending angled or vertical surfaces.
Waiting for the time when the last shall be first and the first shall be last.
The BMJ is patient centred, evidence based, and independent. Help us improve the health of our world with the best science, journalism, education, and comment.
The African Journal of Emergency Medicine (AfJEM) is the official journal of the African Federation for Emergency Medicine.
𝘼𝙣𝙖𝙚𝙨𝙩𝙝𝙚𝙨𝙞𝙖 is the official journal of @assocanaes.bsky.social with comprehensive coverage in peri-operative medicine, critical care and pain.
https://buff.ly/3ARJVrz
#AnSky #MedSky #PainSky #ICUSky #RASky #AirwaySky #PedsAnesSky
Critical care evidence dissemination - science for all.
https://criticalcarereviews.com
The Canadian Journal of Emergency Medicine (CJEM) and the official journal of the Canadian Association of Emergency Physicians (@CAEP_Docs)
Official journal of American College of Emergency Physicians; #1 cited EM research journal
Official account for the 14 American Heart Association Journals covering the breadth of cardiovascular & cerebrovascular disease. When you publish in, review for, or read AHA Journals, you join our fight for a world free of cardiovascular disease & stroke.
The American Heart Journal has been a trusted resource for cardiologists and general practice physicians since 1925.
Editor in Chief: Daniel B. Mark, MD
The JCI is a premiere venue for discoveries in basic and clinical biomedical science that will advance the practice of medicine. Est. 1924