#FOAMed if you want to know how medicine will be practiced #EMIMCC
09.02.2026 17:22 — 👍 3 🔁 0 💬 0 📌 0
+ be aware of undifferentiated shock in extremis (cardiac arrest in seconds) of every morbid condition
20.12.2025 11:42 — 👍 0 🔁 0 💬 0 📌 0
B.D.G.O = Bad Decision Good outcome. Pericolosissimo e sconosciuto
15.12.2025 21:10 — 👍 1 🔁 0 💬 0 📌 0
first:
combination inhaled epo + nitric simultaneously (I know its expensive, put it on my tab)
epi gtt for MAP > 85
to improve cardiovascular reserve if the clot flies off
then:
50 mg tPA
(very little data on IR for clot in transit)
15.12.2025 14:01 — 👍 4 🔁 1 💬 1 📌 0
Great! First glance: add position somewhere (still see patient lying flat)+ I'm unsure if flumazenil deserve any mention. To me the risk is to give any cognitive energy to something which tend to complicate the steps while you need to keep it simple at that point and focus energy on what matters
15.12.2025 20:50 — 👍 1 🔁 0 💬 0 📌 0
@pulmcrit.bsky.social hot take on RSI trial. Again, more questions than answers. But this editorial is amazing and gives you a different view on the trial amongst many other you're about to read in these days. #EMIMCC #FOAMed
14.12.2025 06:24 — 👍 2 🔁 0 💬 0 📌 0
No difference in mortality and such a big gap in CV outcome (surrogates). Something unmesured? #EMIMCC
14.12.2025 06:10 — 👍 1 🔁 0 💬 1 📌 0

article: https://pubmed.ncbi.nlm.nih.gov/37377263/
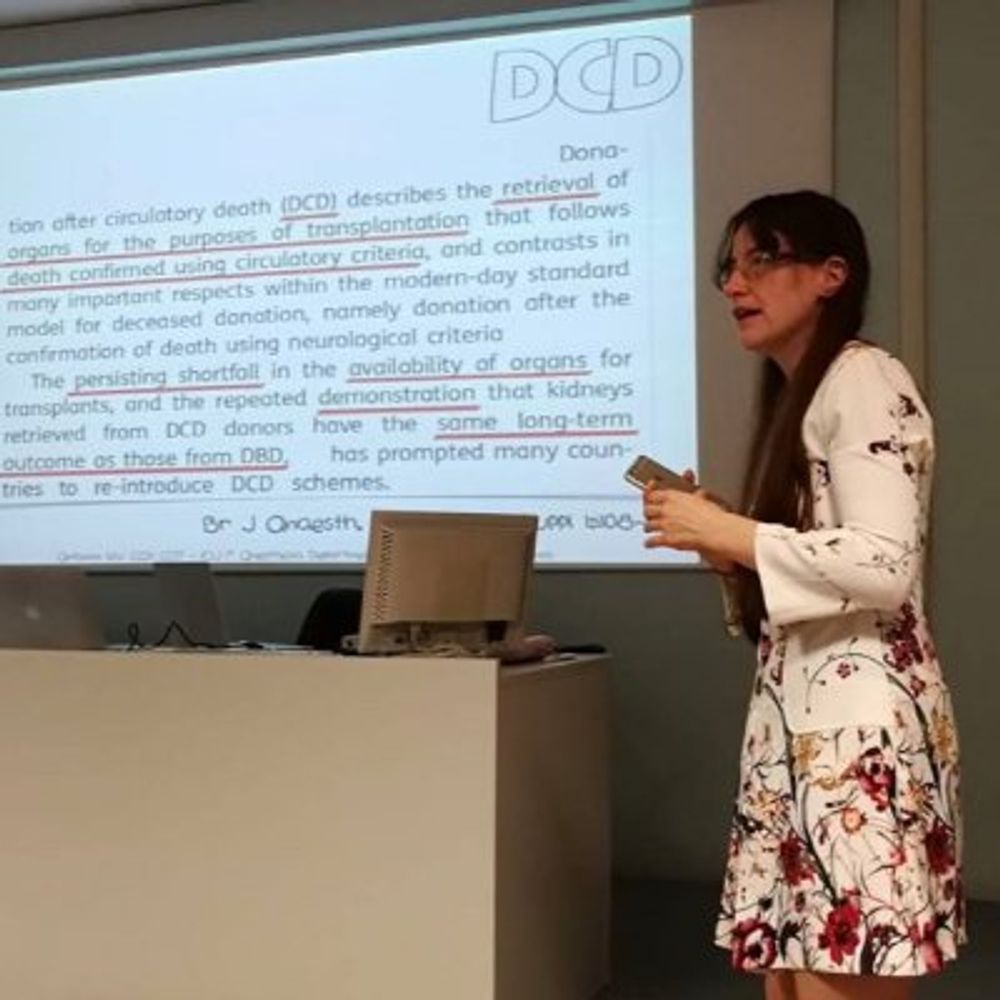
IBCC chapter about acute liver failure: https://emcrit.org/ibcc/alf/
updated the acute liver failure chapter
biggest change is increasing support for early CRRT to remove NH3 (to reduce elevated intracranial pressure)
now rec'd for clinically overt encephalopathy (Grade 2-4)
if admitting to ICU for ALF & encephalopathy, just dialyze
emcrit.org/ibcc/alf/ #EMIMCC
28.11.2025 13:51 — 👍 27 🔁 12 💬 1 📌 1

kermit the frog is wearing a black hoodie and kermit the frog is wearing a black hood .
ALT: kermit the frog is wearing a black hoodie and kermit the frog is wearing a black hood .
PPS - Bottom line is that if your critically unwell patient needs a CT scan you should just get the scan
- Contrast-induced nephropathy is a myth emcrit.org/ibcc/contrast/
- Contrast allergy now just requires a dose of antihistamine
- Radiation risks are minimal (especially for older adults)
18.11.2025 13:51 — 👍 9 🔁 2 💬 0 📌 0
Sooo good
19.11.2025 13:38 — 👍 0 🔁 0 💬 0 📌 0
Already listened to the episode (emcritter here) and I agree. But as it is never a "solo" parameter evaluation, I was wandering if there was another reason to exclude PP, which in some circumstances could be helpfull
18.11.2025 06:14 — 👍 0 🔁 0 💬 1 📌 0
DBP and pulse pressure are somewhat redundant. I added pulse pressure but they will generally trend in opposite directions provided the MAP is held in a somewhat fixed position around 70mm
I guess the evaluation of congestion is kinda assumed... also I wanted to de-emphasize the whole fluids thing
14.11.2025 01:29 — 👍 0 🔁 1 💬 0 📌 0
Why didn't you put in the algorhytm pulse pressure (>40) which was a checkpoint in AS-2?
2) in the rest of the chapter I have not seen a section about fluid tolerance (paired with fluid responsiveness which is present)..is there a reason?
One more time thank you for the IBCC, is a thing of beauty
13.11.2025 05:49 — 👍 1 🔁 0 💬 2 📌 0

Faith, Evidence and the Stars
The most up-to-date critical care website in the world.
"CRT, like a star, is not the destination but a guide for the journey". AS-2 it's not just a trial, it's a manifesto, an act of faith #EMIMCC #Andromeda #AndromedaShock2 #Sepsis
criticalcarereviews.com/blog/current
09.11.2025 21:02 — 👍 1 🔁 1 💬 0 📌 0
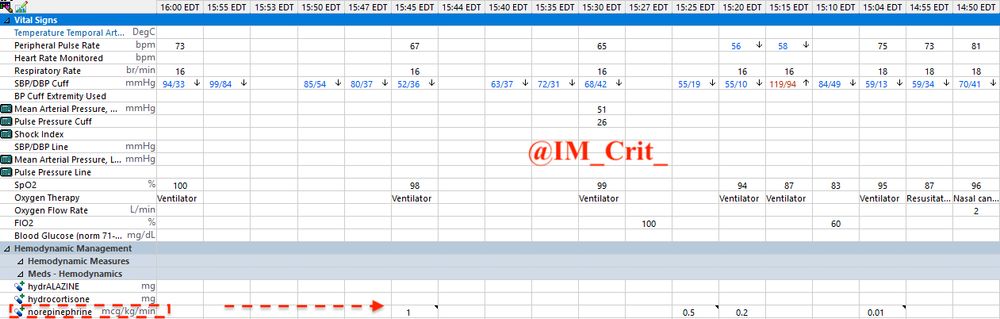
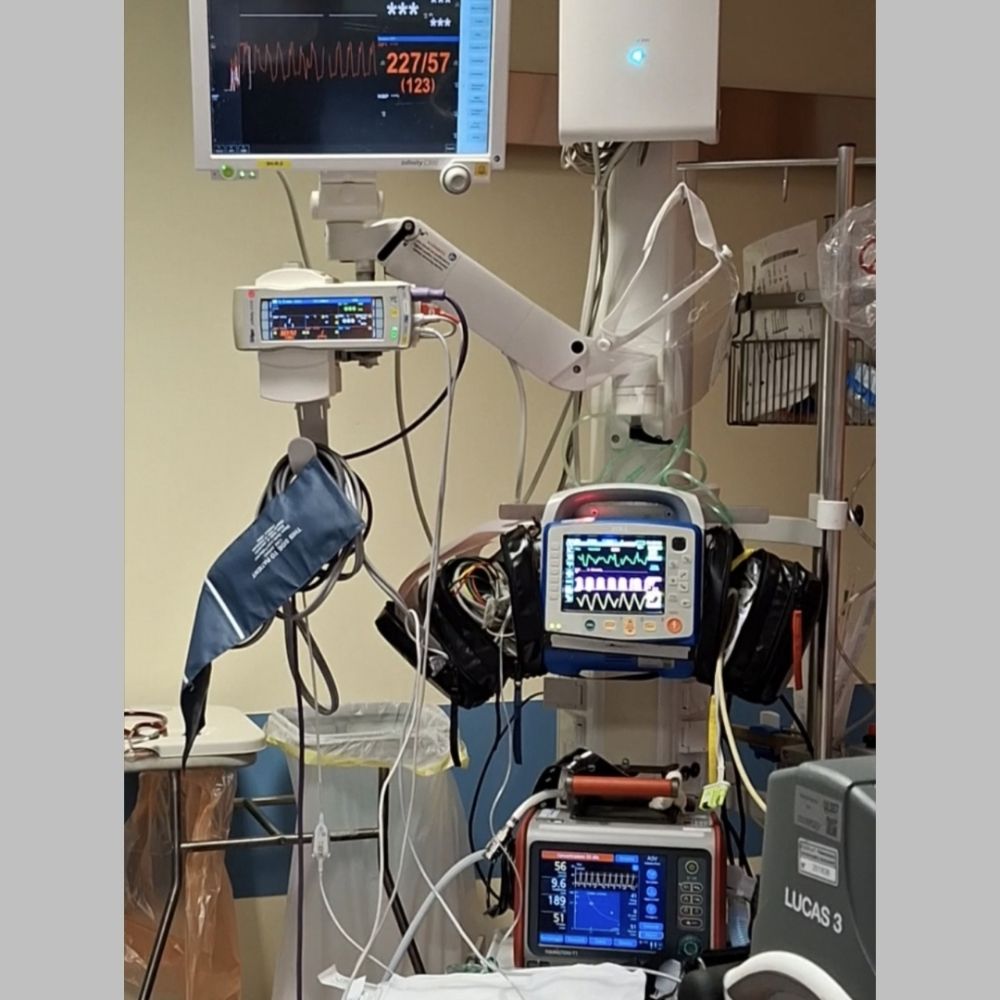
ICU Snapshots:
Young patient with multiple medical problems presented to ED for evaluation of "weakness". Decompensated; had to be intubated & placed on pressors (norepinephrine) before being transferred to our ICU
02.11.2025 19:55 — 👍 7 🔁 1 💬 1 📌 0
BP control can be achieved w sympatholysis and sedation + positive pressure ventilation. I don't see the urgency of put in the mix any antihypertensive med before intubation and I think it's a very dangerous move. If BP high after tubing lets add some drugs. But come on...is not an aortic rupture
27.10.2025 21:05 — 👍 0 🔁 0 💬 0 📌 0

The 2025 European Resuscitation Council Guidelines have been released
All 11 plus the executive summary included below
CCR Journal Watch
https://criticalcarereviews.com/latest-evidence/journal-watch
22.10.2025 12:00 — 👍 9 🔁 5 💬 2 📌 0
but not in a hurry😉
16.09.2025 08:10 — 👍 0 🔁 0 💬 0 📌 0

PLS SHARE. FOR PATIENTS SAFETY SAKE
#EMIMCC
www.tandfonline.com/doi/10.1080/...
11.09.2025 08:09 — 👍 2 🔁 0 💬 0 📌 1
ICU Practice - Return to Basics:
When you prepare for the "average" intubation (no cardiac arrest, no active emesis), how do you pre-oxygenate the patient?
Oxygen mask/nasal cannula?
Non-invasive ventilation?
02.09.2025 21:28 — 👍 8 🔁 3 💬 1 📌 1
ED PHEM doc here. I'm using more and more NIV for preox (usually NIV-ST on Hamilton T1). So I'm giving back up breaths on peep during apneic phase. #EMIMCC
31.08.2025 19:58 — 👍 2 🔁 0 💬 0 📌 0
Give diuretics as boluses
look at Chloride, k+ and pH
Multimodal diuresis
Not every form of "heart failure" need diuretics in the firsts hours
#EMIMCC
#DiuresisJedi
#Deresuscitation
09.08.2025 15:17 — 👍 1 🔁 0 💬 0 📌 0
4. Probably it s better not to try anything "softer" than intubation. But while preoxygenating I d put him on 10 cmh20 of peep at least
03.08.2025 20:30 — 👍 0 🔁 0 💬 0 📌 0
Anyone with similar cases? how did it happen? Just a lack of proper follow up? Some syndromic presentation? It left me kind of unconfortable #EMIMCC is incredibile #FOAMed
31.07.2025 20:47 — 👍 0 🔁 0 💬 0 📌 0
Had a case of elderly M with bilateral carotid stent intubated for sudden collapse and coma. CTA + CTP showed bilateral stent occlusion and complete shut down of anterior brain circulation. Signs of right upper limb ischemia (cold, pulseless). #EMIMCC #FOAMed #Stroke
31.07.2025 20:46 — 👍 0 🔁 0 💬 1 📌 0
A case in which V Tach should be prevented with adrenaline and chronotropism #EMIMCC
28.07.2025 20:27 — 👍 3 🔁 0 💬 0 📌 0
AHAHAHAHAHAHAHA
28.07.2025 11:22 — 👍 0 🔁 0 💬 0 📌 0
@gx8a.bsky.social tu, midazolam team 🤢
22.07.2025 08:35 — 👍 1 🔁 0 💬 0 📌 0
Failing anaesthetist / ICU - now in Registrar flavour. 🏴🇮🇳. 🧠🌶️ 🏳🌈🏳️⚧️ ;
Anaesthetics registrar 💉 ICU inclined 🫁 FRCA 💪 UK trained 🫖 San Francisco 🌈 Physiology fanatic 🫀 Veteran tree-climber 🤸Serial outdoor hobbiest 🚵 Brit in the Bay minded towards better critical thinking and compassion 📚 She/her
Creator of the GMP GUIDE youtube channel, sharing 25 years of pharma experience 💙
https://www.youtube.com/@gmpguide?sub_confirmation=1
I think Pharma knowledge should be free and accessible to anyone.
Open-access, peer-reviewed journal providing an international evidence base to inform improvement in rural and remote health (free to read, no author charges). www.rrh.org.au
#idboardreview #idfellows #idfellowship #IDsky #HIVsky #idmeded
ER doc.
Okay at reading ECGs
Proud to have helped eliminate "excited delirium" in EM.
Aiming to correctly use the subjunctive in Spanish more often.
And I am never, ever sick at sea.
Official account for the 14 American Heart Association Journals covering the breadth of cardiovascular & cerebrovascular disease. When you publish in, review for, or read AHA Journals, you join our fight for a world free of cardiovascular disease & stroke.
ICU Cons + ICS Council. DJ. FUSIC committee ❤️POCUS / FOAMed. Editor: Ox. Handbook of Thoracic Anaesthesia & founder Critical Care Northampton. All views my own
ED Research Registrar (PGY8) at Royal Perth Hospital | Affiliate Researcher at Monash University | Major trauma & EM research. Husband🏳️🌈🇮🇪🇬🇧 views mine
Academic Cardiac and Mobile Anaesthetist | University of Melbourne and Medical School | Medical Director of Sleep Dentistry Services | Day Care Anaesthesia Special Interest Committee
🌐 www.sleepdentistryservices.com.au
📞 0429 058 878
Organic Mechanic | Critical Care Paramedic | Educator | #Airway fanatic | Enthusiastic #POCUS amateur.
Love #POCUS + Blocks + Notfallmedizin, hauptberuflich Beifahrer. (Regional-) Anästhesie, Intensivmedizin, Allgemeinmedizin, Rettungsdienst, #FOAMed, privat hier
emergency medicine, Regional anesthesia, intensive care, general medicine, ambulance service
Fan of all things Science Fiction and Fantasy. Eater of many foods. Failing cyclist and runner. When I have the time Doctor in Emergency Medicine and Intensive Care.
ED physician + TTL in Montreal
EBM | Knowledge Mobilization | Qualitative Research in EM
Anästhesist und Klinischer Akut- und Notfallmediziner aus Rotenburg/Wümme, Ärztlicher Leiter ZNM, FOAMed, Opinions are my own.
Cardiology | #POCUS research | #Echo | #CriticalCare | #Physiology | #Equity | #SDH | #Statistics | #Rstats | #MedSky | #CardioSky | #CCCSky | #emimcc | 🇳🇴🇩🇰 Trondheim, Norway | he/him/han/ham
Emergency Medicine Australasia Journal - keeping you informed about the latest in EM research and topical debates
Perfusionist, E-AEC, ECMO & NRP specialist + POCUS
EuroELSO Steering C & Chair NRP Working Group
ELSOeducation taskforce
SoMe Director @TheELSO
SoMe Editor @asaiojournal
BJHM: An open-access monthly journal dedicated to publishing original investigative and clinical research in hospital medicine. We invite your submission!
Impact Factor: 1.8 | Published by IMR Press
Link: https://www.imrpress.com/journal/BJHM