GLP-1 drugs may provide benefit for idiopathic intracranial hypertension
jamanetwork.com/journals/jam...
jamanetwork.com/journals/jam...

@senolapaydin.bsky.social
Neurologist | Switzerland Emergency Department | Stroke | Neurovascular Ultrasound | Nerve and Muscle Ultrasound | ENMG | Botuliniumtoxin Vienna - Zurich - Basel
GLP-1 drugs may provide benefit for idiopathic intracranial hypertension
jamanetwork.com/journals/jam...
jamanetwork.com/journals/jam...

AANEM Web Lectures on all things ENMG:
youtube.com/playlist?lis...
Great review on everything GBS:
www.nature.com/articles/s41...
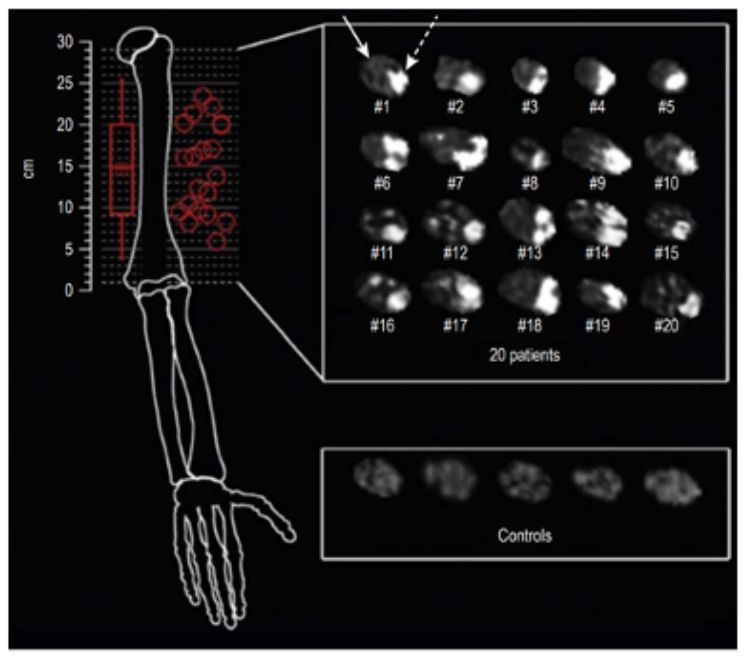
The location of a AIN neuropathy in a Parsonage Turner Syndron is usually at the level of the upper arm:
pubmed.ncbi.nlm.nih.gov/29461642/
Trying to get into neuromuscular ultrasound?
Start here with 'the' expert on this field, Nens von Alfen, via YouTube
youtu.be/vQI3oIVrv44?...
Neurology 🖐️
25.11.2024 19:04 — 👍 1 🔁 0 💬 0 📌 0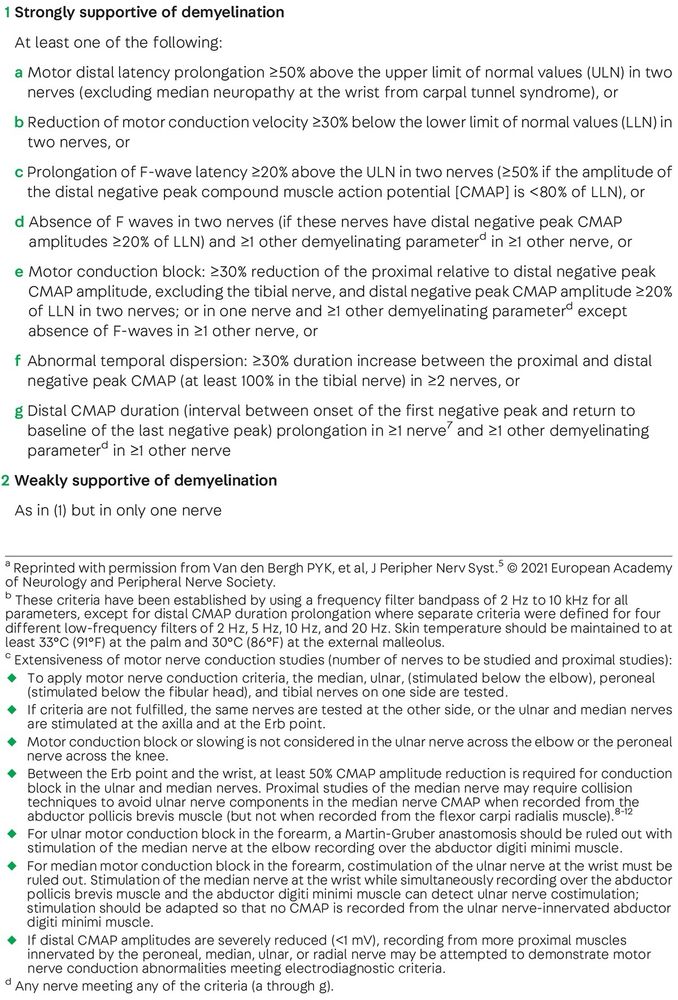
4) Continuum I
Issue, 2023
journals.lww.com/continuum/ab...
3) Neuromuscular Ultrasound in demy. PNP, 2015
pubmed.ncbi.nlm.nih.gov/25691156/
2) Evergreen paper from 2019:
jnnp.bmj.com/content/90/9...

Best ressources on everything #CIDP:
1) EAN Guidelines, 2021
onlinelibrary.wiley.com/doi/full/10....
Back to AIN: Work-up:
1 ENMG
2 Neuromuscular Ultrasound (check for a enlarged nerve)
3 and or MRI
AIN is located in the lower arm, but the pathology is usually a fascicle of the median nerve at the upper arm (check for the lesion with the ultrasound at the upper arm 😉)
So, PA not only as a "Plexusneuritis", can present as a multiplex pattern or mononeuropathy or as pure sensory as well.
22.11.2024 06:46 — 👍 0 🔁 0 💬 1 📌 0Usually affected in the context of a Parsonage Turner (PA):
PA ("Plexusneuritis") commonly at the upper plexus, monophasic, painful onset, later with atrophy (ie scapular winging), motor >>sensory
Most common nerves in PA:
Thoracic longus
Supra-/ Infraspinatus
AIN
PIN
AIN Neuropathy:
AIN: Anterior interosseus nerve (median nerve), pure motor (!) nerve (branching off on the upper part of the lower arm) supplying
1 flexor digitorum profundus II/III (distal finger Flexion)
2 flexor pollicis longus (distal thumb flexion) and
3 pronator quadratus (handpronation)
 21.11.2024 22:26 — 👍 1 🔁 0 💬 0 📌 0
21.11.2024 22:26 — 👍 1 🔁 0 💬 0 📌 0
ENMG work-up:
1 APB motor and sensory plus f-waves
2 ADM motor and sensory plus f-waves (DD PNP)
3 Radial sensory (DD Plexus)
(4 Pronator quadratus motor DD AIN)
If any other median hand muscle is affected?
Flexor digitorum profundus II/III and Flexor pollicis longus are supplied by the AIN (proximal median neuropathy). Not affected in CTS. AIN usually in the context of a Parsonage Turner Syndron. AIN has no sensory branch, thus no sensory impairment.
Motor: Weakness of the LOAF muscle
Lumbricalis
Opponens pollicis
Abductor pollicis brevis (APB)
Flexor pollicis brevis
Usually the APB is tested. No other muscle but the LOAF muscle is involved in CTS.
Preparing for the #ENMG boards 😅
How to work up a hand numbness? Most likely? #CTS.
Typical Symptoms: Pain at night (which can spread up to the upperarm).
Sensory: Dig I -IV (with ulnar split). Thenar is spared. Why? Palmar branch, which supplies the thenar, does not pass the carpal tunnel.
So true! I used to listen in while preparing for the boards 🤓
17.11.2024 16:56 — 👍 2 🔁 0 💬 0 📌 0Stroke Guidelines 2024, Bern
neurologie.insel.ch/fileadmin/Ne...
Neurology Exam Prep Podcast:
www.buzzsprout.com/798455
 16.11.2024 21:51 — 👍 1 🔁 0 💬 1 📌 0
16.11.2024 21:51 — 👍 1 🔁 0 💬 1 📌 0
 16.11.2024 21:51 — 👍 2 🔁 0 💬 1 📌 0
16.11.2024 21:51 — 👍 2 🔁 0 💬 1 📌 0
 16.11.2024 21:51 — 👍 2 🔁 0 💬 2 📌 0
16.11.2024 21:51 — 👍 2 🔁 0 💬 2 📌 0
Highly recommended ressources in the field of neurology, ⭐⭐⭐⭐⭐
16.11.2024 21:51 — 👍 3 🔁 0 💬 2 📌 1