First thought: neuro twaves. But sounds like i was wrong…darn it.
29.04.2025 04:56 — 👍 1 🔁 0 💬 0 📌 0
what Swami is referring to here is a “bolus” but given as a slow infusion over a period of time. Theres RCT evidence that says it reduces psychomimetic rxns versus pushing it over a few minutes
25.04.2025 01:10 — 👍 0 🔁 0 💬 0 📌 0
Interesting question and context. In the ED i tend to give a bolus then start a drip. In the ICU i just start the drip. No particular reason, you just made me self reflect 🤷🏻♂️
Important to be clear what “infusion” means bc even giving a single dose of 0.3 should be done over 15-20 mins to reduce SE
25.04.2025 01:10 — 👍 0 🔁 0 💬 1 📌 0
Oh buddy!
This job is just a maze of booby traps. Crazy
23.03.2025 22:04 — 👍 1 🔁 0 💬 0 📌 0


ICU Stories:
Elderly patient with multiple medical problems (HFpEF / A fib / HTN / PE / obesity etc) was admitted w CHF exacerbation. Improved w diuresis but developed left upper extremity edema; diagnosed with extensive DVT for which Interventional Radiology (IR) was consulted
22.03.2025 18:59 — 👍 34 🔁 6 💬 1 📌 0
I love this. I see this from time to time with a bariety of triggers. Maybe an HLH spectrum phenomenon. Super interesting. Ive had some luck with Methylene blue or B12 on a couple occasions.
23.03.2025 15:37 — 👍 2 🔁 0 💬 0 📌 0
Awesome stuff. Loads of great info here. Thanks!
16.03.2025 18:05 — 👍 1 🔁 0 💬 0 📌 0

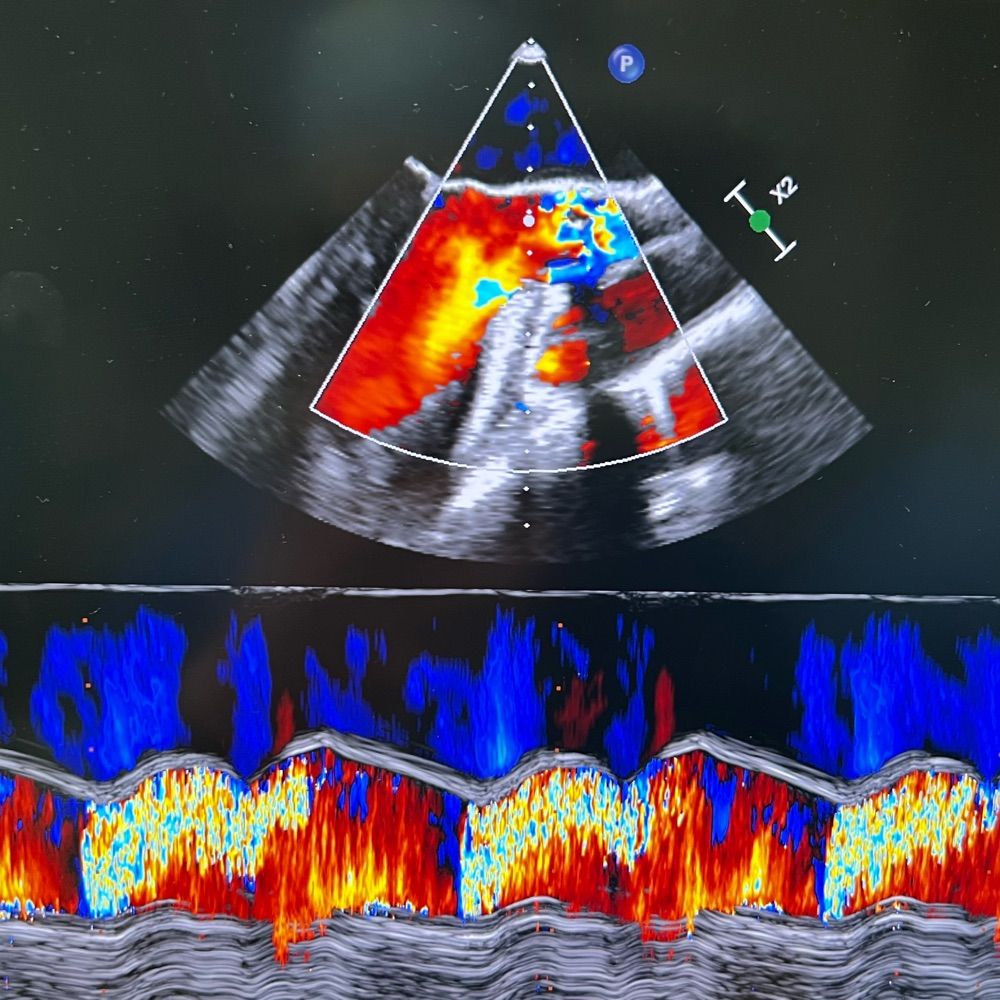
ICU #POCUS:
This is a recently published, information-dense document. It may be a bit technical for the average POCUS user but if you manage patients who harbor a right heart (😊), consider reading it:
16.03.2025 03:00 — 👍 20 🔁 5 💬 1 📌 0
Im just gonna leave a little chuckle here bc this is so true and so common 🤣
16.03.2025 02:42 — 👍 1 🔁 0 💬 0 📌 0
This cannot be over emphasized. If you just titrate this slowly to your goal it takes forever.
16.03.2025 02:41 — 👍 0 🔁 0 💬 0 📌 0
Dude totally agree. I wqs a little tachycardic during that scene. ive seen this twice now. This is not the EPi and high fives scenario. This is put the tube in and wait it out. This goes badly fast.
16.03.2025 01:10 — 👍 1 🔁 0 💬 0 📌 0
I like this. At least by ultrasound. You can get away with using inotropes +\- diuretics but honestly if things dont turn around real quick (lactate, UOP, etc) i strongly believe you need some data. Whether thats pocus or PAC or even Ficks w an ScV02 whatever. I agree with you here.
16.03.2025 01:07 — 👍 1 🔁 0 💬 0 📌 0
Agree wholeheartedly 💪🏼
01.03.2025 08:41 — 👍 2 🔁 0 💬 0 📌 0
YouTube video by Peter Johns
Syndromic vs diagnosis based approach to dizziness/vertigo: Which is better?
Great video from Dr Peter Johns detailing the syndromic vs diagnosis based approaches to vertigo in the ED #emimcc
youtu.be/e9Qcuzi3m6Q?...
28.02.2025 07:48 — 👍 7 🔁 1 💬 0 📌 0
💯%
Lots of em😂
26.02.2025 05:07 — 👍 1 🔁 0 💬 0 📌 0
A quick #VEXUS thread 🧵-
3 reasons why the portal vein is the most useful single venous doppler waveform 🥇
(if you're only going to do ONE site to look for venous congestion, this is probably the most useful one!)
#emimcc
25.02.2025 18:30 — 👍 21 🔁 14 💬 3 📌 0
Well. I think i hear ya.
But Flu = CAP. Many (most?) CAP is viral, flu is a common pathogen.
So youre saying lobar consolidations, elevated procal etc youre using steroids, but diffuse GGOs, lower procal, but still sick, no.
Thats reasonable honestly, just seems like a lot of overlap.
26.02.2025 04:28 — 👍 0 🔁 0 💬 1 📌 0
Very rational. I mean, theres quite a few observational studies that are consistent, despite the fact that none are controlled. Not exactly cause and effect type science but consistent observations in various settings strengthens a hypothesis, right?
26.02.2025 04:25 — 👍 1 🔁 0 💬 2 📌 0
Oh boy 🤦🏻♂️
26.02.2025 04:20 — 👍 0 🔁 0 💬 0 📌 0
So not up front huh? Just when things are getting worse despite standard treatments? Reasonable.
24.02.2025 03:53 — 👍 1 🔁 0 💬 1 📌 0
Right? I mean pooled data on very heterogenous groups of lung injury seem to benefit and until theres some prospective data or at least a tested mechanistic hypothesis (?innate immunity to recurring exposure to seasonal flu?) as to why its different I cant imagine it would be exempt 🤷🏻♂️
24.02.2025 01:01 — 👍 1 🔁 0 💬 1 📌 0
#foamed #foamcc #meded #medsky #idsky #emimcc #cccsky @imcrit.bsky.social @pulmcrit.bsky.social @nickmark.bsky.social @emcrit.bsky.social @zentensivist.bsky.social
23.02.2025 22:01 — 👍 1 🔁 0 💬 1 📌 0

homer simpson is standing in a grassy field
ALT: homer simpson is standing in a grassy field
So during this bad flu year with the many people we are putting on IMV and even VVECMO, knowing that theres no updated evidence for FLU+ patients specifically….
Are we using steroids for severe CAP or ARDS in FLU+ patients?
Disclosure: I have been 🤫 🤐
23.02.2025 22:01 — 👍 0 🔁 0 💬 3 📌 0
IDSA/ATS still recommends against steroids in FLU+ patients.
CAPECOD excluded FLU+ pts.
Yet many severe CAP and ARDS are caused by FLU and a non trivial number of them are c/b bacterial PNA.
23.02.2025 22:01 — 👍 4 🔁 0 💬 1 📌 0
Ok team. Rubber meets the road
Its a bad flu year so we have to talk about it.
We have CAPE COD trial, and updated guidelines for steroids in CAP, and a shift toward erring on the side of using steroids for CAP and ARDS
Traditionally based on observational data alone steroids not rec’d in FLU+ CAP
23.02.2025 22:01 — 👍 8 🔁 1 💬 1 📌 0
I use it a lot. Anecdotally it seems to be less sedating and probe to side effects than the antihistamine/anticholinergic versions of “msk relaxers”
I use to use it routinely in trauma pts and msk related pain but i dont see those pts much these days
13.02.2025 17:05 — 👍 0 🔁 0 💬 0 📌 0
Cool review. Good on the authors. I was hoping they would delve into the catheter based therapies evidence or lack thereof (the big black box) but i did think it was cool they brought up VAECMO. Good stuff.
13.02.2025 01:41 — 👍 1 🔁 0 💬 0 📌 0
Wow. Ibutilide. What a concept. Ive never given it. Good point though about aaF in the ICU vs ED. Different disease practically. Its kind of fun in the ED, kind of a bane in the ICU. Thx for the recommendation ill have to look further into that.
12.02.2025 02:48 — 👍 3 🔁 0 💬 0 📌 0
Another scenario may be when you have VAECMO and an impella in, your PAC estimates of CI are kind of unreliable so was wondering if VTI + flows from MCS devices may be the way. Gets tricky ya know.
12.02.2025 00:50 — 👍 2 🔁 0 💬 0 📌 0
leading monthly multi-specialty journal for hospital doctors and other healthcare workers.
Link: https://magonlinelibrary.com/journal/hmed
Email:lydia@bjhmhealth.com
Military | Physician-Scientist | Emergency Medicine 🚑 | Critical Care | X @armyemdoc | Instagram @armyemdoc | My views/opinions only, not medical advice
EM physician | POCUS | ECG | Med edu | FOAMed.
Emergency Medicine Australasia Journal - keeping you informed about the latest in EM research and topical debates
Cardiothoracic and Vascular Anaesthetist and Intensivist
ECMOology, Echo, Critical Care Transfer and Cats
Not in that order
Critical Care | Emergency Medicine | Trauma | POCUS | Healthcare Absurdity
Emergency physician & Dean of the Yale School of Public Health. Gun violence prevention researcher. Incorrigible optimist (because we can and do create change, together). Mom of two teens. GO BILLS. @meganranney at the other place 🛟🩺📉📈🧪
EM Pharmacist & Hockey Goalie & Travelist | Living & appreciating life to the fullest | Sharing what I learn everyday. Opinions are my own, RTs not endorsements #MedSky #EMsky #PharmSky
Pulm/CCM, Arsenal, travelling. Meded. FOAMed
Card game for MedEd
MedEd games research
Podcasting at PedsRAP
Pediatrics in PDX IRL
Typos retained as proof of human authorship
https://podcasts.apple.com/mr/podcast/academic-pediatrics-podcast/id1316140783
EmpiricGame.com
Editors: Josef Trapani & Peter Nydahl
Official Journal of the British Association of Critical Care Nurses
https://onlinelibrary.wiley.com/journal/14785153
Academic Hospitalist MD | APD IM | Interests-pt safety, QI, POCUS, faculty development, meded, pain mgmt, & obesity. Carbs, ice cream, Diet Coke and cold brew lover. Cinephile-wrote thesis on Almodóvar. Fred the auggie=perrijo. Polyglot.
Advancing lung health through innovative education, clinical excellence, and groundbreaking research. Visit https://www.chestnet.org to learn more.
June 4-5, 2025 (for Trainee); June 4-6, 2025 (for Faculty) #CCCES25
https://med.umn.edu/divisions/cardiovascular/Critical-Care-Cardiology-Education-Summit
🤝Bring critical care cardiologists together to build a community and train FITs interested in CCC.❤️
The Society of Critical Care Medicine (SCCM) is the largest non-profit medical organization dedicated to promoting excellence and consistency in critical care.
Account maintained by Konrad Jacobs
👉 Glyn Williams: Consultant in Paed Anaesthesia / Pain Management; Clinical lead, Pain Management Service, GOSH
👉 Konrad Jacobs: Consultant Clinical Psychologist; Lead, Oxford Centre for children and young people in Pain
EM & trauma physician | I use simulation to design better healthcare systems and spaces | Founder, Advanced Performance | otherwise @eagles & @raptors
Critical Care and Emergency Physician, passionate about understanding and explaining abnormal physiology
EM Physician+Educator+Pt Advocate // emdocs.net EIC & Co-founder // #EMRA45u45 // #GirlDad // #citizenofworld // #selfmade