Great case @rkchoi.bsky.social !!!
06.09.2025 21:37 — 👍 1 🔁 0 💬 0 📌 0


1/ Hello #medsky #neurosky #neurocritcare #FOAMEd have another brief case that I wanted to discuss with you and see if maybe you can learn something new or reinforce old knowledge!
03.09.2025 20:00 — 👍 7 🔁 4 💬 1 📌 0

Heading to #AANAM? The NDEC #secretmission continues with another chance to win the glial gladiator belt.
Join @caseyalbin.bsky.social @jrgoldstein.bsky.social & @drjmartindale.bsky.social Sunday 4/6 for a digital technology tour & receive your mission instructions! #neurosky
04.04.2025 13:46 — 👍 6 🔁 3 💬 0 📌 1
Join the #secretmission and learn more tomorrow at 7AM for a Technology Tour in the @aanmember.bsky.social education room with @caseyalbin.bsky.social, @drjmartindale.bsky.social and @jrgoldstein.bsky.social
05.04.2025 17:39 — 👍 5 🔁 4 💬 0 📌 0
Do you care for pts with disorders of consciousness in any capacity (as a MD, RN, social worker, pharmacist, PT, OT, caregiver etc!!)?
👇5 min survey on what educational resources you'd like to see Neurocritical Care Society provide?
04.03.2025 02:46 — 👍 2 🔁 3 💬 1 📌 0
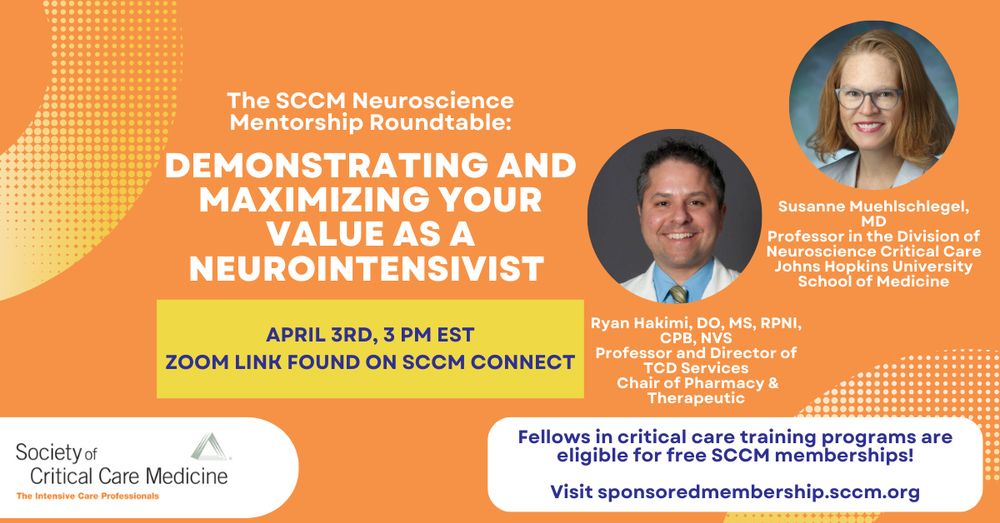
Curious about RVUs, want to know if you are billing correctly, how about diversifying your revenue stream??
We've got answers from @smuehlsch.bsky.social & Dr. Ryan Hakimi.
Save the date!
The zoom link is on SCCM connect and will be emailed if you are part of the neuroscience section
11.03.2025 20:22 — 👍 5 🔁 3 💬 1 📌 0
Was so fun to join you!!!
13.03.2025 20:14 — 👍 1 🔁 0 💬 0 📌 0
Hmm like beyond ENLS?
11.03.2025 21:34 — 👍 0 🔁 0 💬 1 📌 0
Curious about RVUs, want to know if you are billing correctly, how about diversifying your revenue stream??
We've got answers from @smuehlsch.bsky.social & Dr. Ryan Hakimi.
Save the date!
The zoom link is on SCCM connect and will be emailed if you are part of the neuroscience section
11.03.2025 20:22 — 👍 5 🔁 3 💬 1 📌 0
@ericclawsonmd.bsky.social @aartisarwal.bsky.social @drdangayach.bsky.social @hehinson.bsky.social @danharrisonmd.bsky.social @richardchoi.bsky.social
04.03.2025 02:46 — 👍 0 🔁 0 💬 0 📌 0
Do you care for pts with disorders of consciousness in any capacity (as a MD, RN, social worker, pharmacist, PT, OT, caregiver etc!!)?
👇5 min survey on what educational resources you'd like to see Neurocritical Care Society provide?
04.03.2025 02:46 — 👍 2 🔁 3 💬 1 📌 0
Bookmarked for our travel day tmw!!
Critical work to define entrustment in NeuroICU APPs!
02.03.2025 23:53 — 👍 3 🔁 0 💬 0 📌 0
Mark your calendars for Sunday!!
Come hang with all the brain nerds😎 in Orlando!
Help spread the word!
@aartisarwal.bsky.social @drdangayach.bsky.social
blob:null/88bed75b-9775-438b-89fb-0597d2f80f4c
20.02.2025 12:36 — 👍 3 🔁 2 💬 0 📌 0

Are we missing cases of ocular telangiectasia and ataxia (walking and coordination) syndrome? YEP. Should these folks avoid X-rays? YEP. Do you know what features these cases may present with at ~age 40. Lukas Gattermeyer-Kell and colleagues show us two key images and teach us all about it.
26.01.2025 13:41 — 👍 16 🔁 1 💬 0 📌 1
I think this is a reasonable take based on the evidence!
Do I really think the grade 1 SAH with a whisp of blood and low risk of DCI needs a Hgb of 9? No.
But for pt in clear vasospasm (aSAH but also TBI) or other perfusion disturbing physiology I think I will keep 9 as my threshold.
10.12.2024 21:52 — 👍 4 🔁 0 💬 0 📌 0
18/
Interested in how others are interpreting these results. Again, huge congrats to the authors. and a special shout out to Dr. Ofer Sadan who led the SAHARA effort at
@emoryneurocrit.bsky.social
@ericclawsonmd.bsky.social @pulmcrit.bsky.social @aartisarwal.bsky.social @ajwpharm.bsky.social
10.12.2024 18:30 — 👍 8 🔁 0 💬 2 📌 0

a showtime ad for billions shows an old man talking to another man
ALT: a showtime ad for billions shows an old man talking to another man
17
I think there is enough data to suggest that aiming for 9g/dL PARTICULARLY (maybe exclusively) in pts at ⬆️ risk for decreases in cerebral perfusion due to ongoing physiologic changes like vasospasm makes sense given the control population in this trial & the results of TRAIN
10.12.2024 18:30 — 👍 6 🔁 1 💬 1 📌 1
16/
The way I have put this together, is that I will be more aggressive (than the standard 7 or what we have allowed as 8g/dL) in transfusions for the patients at highest risk for secondary neurologic injury.
10.12.2024 18:30 — 👍 4 🔁 0 💬 1 📌 0
15/
It seems to me a take away is that 10g/dL is too high to offer benefit, but the lowest acceptable number I think is still up for debate, and TRAIN would suggest 9g/dL might be a more reasonable target.
Indeed, the restrictive group in SAHARA was on average > that threshold
10.12.2024 18:30 — 👍 4 🔁 0 💬 1 📌 0

14/
In other neurocritically ill pts including SAH (the recently published TRAIN trial), we did reduce unfavorable outcomes when we set the "liberal" threshold of <9g/dl and restrict all the way down to <7g/dl. This looked at 6 month outcome.
10.12.2024 18:30 — 👍 5 🔁 0 💬 1 📌 0
13/
This trial was very well done and is pragmatic and generalizable.
The threshold of 10 doesn't seem to improve neurologic outcomes.
However, I don't look at this trial and think that we conclude that maintaining a daily hgb of 8g/dl is proven ok.
10.12.2024 18:30 — 👍 5 🔁 0 💬 1 📌 0

12/
Between these two groups, there was no significant difference in mRS at 12 months and the risk of having a poor outcome.
10.12.2024 18:30 — 👍 4 🔁 1 💬 1 📌 0

11/
Note also that once the liberal group got transfused they also mostly stay well above even the liberal threshold.
So intervention was transfusion for a low threshold of 8g/dl ... but we're I think ultimately comparing outcomes for avg daily hgb of ~11g/dL to ~9.5 g/dL
10.12.2024 18:30 — 👍 3 🔁 0 💬 1 📌 0
10/
However, while the two group are clearly different, its important to note... the restrict group was on avg above 9 g/dl.
Said differently the controls were anemic, but did not linger 8g/dL threshold... so, the intervention, if needed, got them well away from the "danger" level
10.12.2024 18:30 — 👍 3 🔁 0 💬 1 📌 0

9/
The median time before enrollment was 3 days (meaning by day 3 the hgb dropped below 10). this is important as it is right before patients would enter the period of highest risk for vasospasm and DCI. And the separation of hgb levels was well differentiated between the groups
10.12.2024 18:30 — 👍 3 🔁 0 💬 1 📌 0
8/
The groups were well matched in terms of gender, age, WFNS scale, modified Fisher grade. Most had anterior circulation aneurysms, and most were rapidly treated endovascularly.
Radiographic vasospasm was seen in 36.6% of liberal strategy and 35% of restrictive strategy pts
10.12.2024 18:30 — 👍 3 🔁 0 💬 1 📌 0

a woman is smiling and saying `` they 're all so different '' while standing in front of a brick building .
ALT: a woman is smiling and saying `` they 're all so different '' while standing in front of a brick building .
7/
Everything else about the management was determined per the treating team.
And remember, there is variability between institutions about BP goals, how frequently IA is performed, how DCI is screened for, and how meds like milrinone and intrathecal nicardipine are used.
10.12.2024 18:30 — 👍 3 🔁 0 💬 1 📌 0
6/
And given this and other studies on the importance of anemia avoidance, surveyed neurointensivists, neurosurgeons, and intensivists felt that a threshold of 8g/dL was a more acceptable lower limit than waiting until 7g/dL to transfuse.
So 8 it is.
10.12.2024 18:30 — 👍 3 🔁 0 💬 1 📌 0

The Effect of Packed Red Blood Cell Transfusion on Cerebral Oxygenation and Metabolism After Subarachnoid Hemorrhage - PubMed
PRBC transfusion resulted in PbtO2 improvement without a clear effect on cerebral metabolism prior to SAH.
5/
wait wait wait.... in other critical care situations we use a threshold of 7g/dL for transfusion... why wasn't this the threshold?
Because prior studies have suggested anemia adversely affects cerebral oxygenation and metabolism after aSAH.
pubmed.ncbi.nlm.nih.gov/26195087/
10.12.2024 18:30 — 👍 3 🔁 0 💬 1 📌 0
Vascular Neurology /StrokeNet fellow at UTHouston; #Meded #Medsky #Neuro #Neurology #Stroke
ID MD @EmoryMedicine.
Interested in educating the next generation of learners using and supporting clinician-educators. Science of learning, curriculum development, instructional methods, #MedEd research, #SoMe Ed, visual design.
Hospitalist, VA Boston Healthcare System. Co-host, Curious Clinicians Podcast
Hospitalist and Health Services Researcher at SFVA | Assoc. Prof of Medicine at UCSF | Senior Deputy Editor for Journal of Hosp Med | Director of SFVA VA Quality Scholars program | Proud dad and avid cyclist
General IM doc focused on improving #MedEd and #HPE through #ProfessionalDevelopment and access to #Mentorship. CEO and co-founder of @MedEdMentor. My posts represent my own opinions and not those of my employers. #MedSky
Physician, educator, historian, author, podcaster, researcher at Beth Israel Deaconess Medical Center and Harvard Medical School, host of histmed podcast Bedside Rounds, associate editor at NEJM AI, studies 🤖+🧠. 🖖🚲
EM physician interested in MedEd, training the next generation of EM docs who can practice EM anywhere, anytime, and take care of anything. Side projects include woodworking, cooking some good food here and there, and making things grow in the garden
PhD Medical and Health Professions Educator at the Saint Louis University School of Medicine. #MedEd
https://www.slu.edu/medicine/about/faculty-resources/cedar/index.php
Proceduralist/Hospitalist/APD | #MedEd #MedSky #IMPOCUS | Son 🇮🇳 & Husband 🇬🇧 of Immigrants | 🍺🌮✈️🌍⚽️🏈 | #GirlDad | Ally | Views≠Employer’s
The open-access, MEDLINE-indexed journal of teaching and learning resources published by the AAMC. #MedEd #FOAMed #MedSky
https://www.mededportal.org/
Saying the product of the kidneys is urine is like saying the product of a factory is pollution. Urine is a by-product. The product is homeostasis.
COI: https://pbfluids.com/about/
Founding Dean & VP Medical Affairs @TorontoMet School of Medicine by Day, EM doc by night
Alumni: UofT SchulichMedDent MacEmerg UICdme UofPeople #MedEd #FOAMed #MedSky
Neurologist, NeuroID, neuroimmunologist, medical educator @ University of Alabama at Birmingham
Wife, Mom, work life juggler. Posts are my own.
Neurologist. Interested in prehospital emergency medicine, critical care, stroke, neuroethics. Views my own. She/her. #NeuroNerd #WomenInMedicine
Assistant Professor of Vascular Neurology @NYULangone @BellevueHosp | former @pennmedicine.bsky.social
Stroke Neurologist. The brain is fascinating 🧠
We strive to provide outstanding clinical care, train leading neurologists and scientists of the future and to serve as an international leader in Neurology.
neurology.washu.edu
Autoimmune Neurologist at Mayo Clinic, Personal account