🧵 1/ NHS England’s Fit for the Future 10-Year Plan is set to transform postgraduate medical education. Flexibility, digital platforms & modular learning sound great, but what’s at stake? @drlkvaughan.bsky.social & I ask some important questions in a new paper in J Roy Soc Med
02.12.2025 18:10 — 👍 5 🔁 5 💬 1 📌 0
@trishgreenhalgh.bsky.social @drrachelclarke.com @kitb.bsky.social
26.11.2025 11:20 — 👍 3 🔁 0 💬 0 📌 0

Medical education at the crossroads. Part I: undergraduate education and the erosion of professional identity - Louella Vaughan, Martin McKee, 2025
What's the future for Undergraduate Medical Education in England?
@martinmckee.bsky.social and I look at what's in the 10 Year Plan and the implications.
We think there is significant risk of the proposals devaluing degrees and the Profession.
journals.sagepub.com/doi/10.1177/...
26.11.2025 11:20 — 👍 6 🔁 6 💬 1 📌 0
👇… Not right time for vote / when done - do properly! ….
28.09.2025 17:33 — 👍 1 🔁 1 💬 0 📌 0
@martinmckee.bsky.social @drrachelclarke.com @parthaskar.bsky.social @trishgreenhalgh.bsky.social
28.09.2025 17:19 — 👍 0 🔁 1 💬 0 📌 0

RCP Constitutional Reforms - The Case for No (Not Yet)
The Royal College of Physicians (RCP) is currently asking Fellows to vote on constitutional reforms. The reforms seem relatively straightforward – widening the franchise to allow Collegiate members to...
The RCP is asking Fellows to vote on key constitutional reforms, including extending the franchise.
A group of 27 Fellows tabled a motion saying reform should be slowed down + done properly.
Not enough information. Too many questions.
Our views here:
tinyurl.com/ye5k2fa2
28.09.2025 17:19 — 👍 10 🔁 4 💬 1 📌 1
Interesting piece Helen!
21.08.2025 16:30 — 👍 0 🔁 0 💬 0 📌 0
😁
01.08.2025 13:24 — 👍 1 🔁 0 💬 0 📌 0
Sadly, you are probably right.
To be subdivided and flogged for apartment blocks.
01.08.2025 13:24 — 👍 1 🔁 0 💬 0 📌 0

This is mine!
01.08.2025 13:21 — 👍 1 🔁 0 💬 1 📌 0
Lovely! Lucky you.
01.08.2025 13:19 — 👍 1 🔁 0 💬 1 📌 0
Australian 3/4 acre block outer suburbs...
01.08.2025 13:17 — 👍 0 🔁 0 💬 1 📌 0
Andy, this topic is MUCH more fun over on Twitter.
Everyone on Bluesky is too polite.
10.07.2025 10:53 — 👍 1 🔁 0 💬 0 📌 0
I am so very sorry Trisha.
She was a very lovely one.
19.04.2025 13:26 — 👍 1 🔁 0 💬 0 📌 0
Time is running out!
Less than 3 days left to vote in the @rcphysicians.bsky.social elections.
Links to voting in email from Civica.
Vote @drlkvaughan.bsky.social for Vice President!
11.04.2025 13:43 — 👍 3 🔁 2 💬 0 📌 0
Please encourage your FRCP colleagues to vote before Monday 14th April
Vote Asif Qasim for President
@drlkvaughan.bsky.social for VP
@respirologist.bsky.social Dr Philip Pearson for Council
@copddoc.bsky.social Prof Nick Hopkinson for Council
#TimeForChange
10.04.2025 17:15 — 👍 7 🔁 4 💬 2 📌 0
Thanks both!
Claudia and I found it a very difficult piece of work to do. But was important to document experiences and analyze impact soon after events.
Organisations have VERY short memories.
08.04.2025 10:30 — 👍 1 🔁 0 💬 0 📌 0
I've talked to hundreds of Members and Fellows and their views are clear: we need to revitalise the RCP and restore the #VoiceOfPhysicians
Vote Asif Qasim before Monday 14th April
It's time to act: let's make the RCP something we can be proud of
02.04.2025 13:14 — 👍 7 🔁 6 💬 2 📌 1
Thanks Fiona!
The algorithm threw you up in my timeline on pretty much my first day on Twitter.
I thought: Oh Cool. Interesting stuff. And followed you.
Here we are, a decade later...
02.04.2025 09:19 — 👍 1 🔁 0 💬 0 📌 0
Governments around the world need to face up to the issue that the cost of providing healthcare over the next 2 decades is going to be wildly expensive.
Making the workforce less skilled and less efficient for marginal cost savings isn't the solution.
Fin
01.04.2025 13:45 — 👍 2 🔁 1 💬 1 📌 0
half a century. Fully trained doctors provide the best care. It just isn't possible to chunk up the job and outsource it.
Not is it just not efficient in the long run, but it creates other problems. And patients suffer as a consequence.
5/
01.04.2025 13:45 — 👍 0 🔁 0 💬 1 📌 0
How do you make one?
How do you ensure safety and accountability?
Especially problematic given that what doctors do (mostly) is to THINK about things and make DECISIONS. The skill stuff is an added extra.
The grand experiment with workforce subs has been going on for over
4/
01.04.2025 13:45 — 👍 0 🔁 0 💬 1 📌 0
that not everything a doctor does need years of training. And somethings could (and have been been) be safely done by someone not a doctor.
But the problem is that workforce substitution quickly slides into the existential:
What is a doctor?
What do they do?
3/
01.04.2025 13:45 — 👍 0 🔁 0 💬 1 📌 0
anywhere in the world. Except perhaps Germany.
The logical solution is train more doctors and to use carrots (+ the occasional stick). But this is expensive!
So the alternative, since the 1960s, has been workforce substitution. This is attractive, as it certainly is true
2/
01.04.2025 13:45 — 👍 0 🔁 0 💬 1 📌 0
Just off the Leng Review call.
Once again it strikes me just how existential the issue of workforce substitution is and what is at stake.
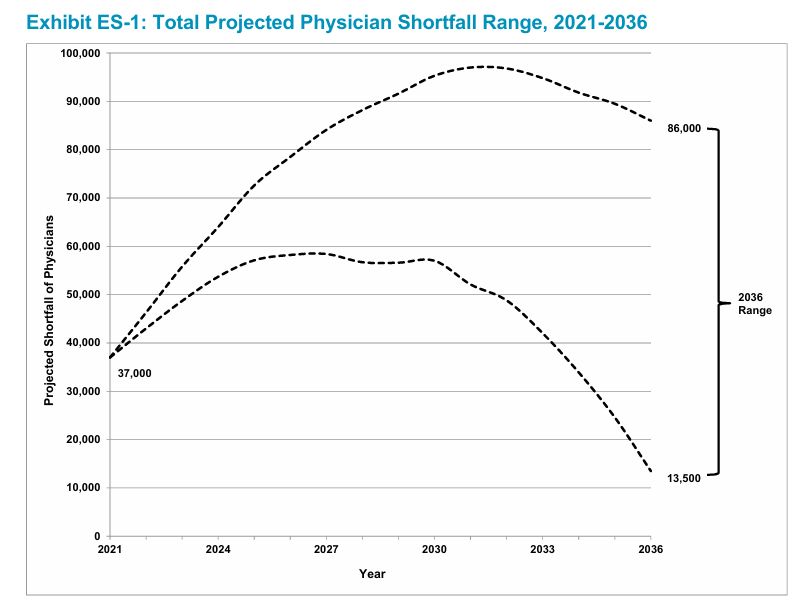
The root cause is not enough doctors. Historically, not enough in rural and remote places. With the coming 'Silver Tsunami', not enough
1/
01.04.2025 13:45 — 👍 0 🔁 0 💬 1 📌 0
Why Does This Matter?
Because for the last decade or so, health policy has been led by superficially appealing. but unevidenced ideas and *vibes*.
The only way out is evidence and clear thinking.
The RCP needs to become a powerhouse for evidence-based policy.
Fin.
01.04.2025 10:21 — 👍 2 🔁 1 💬 0 📌 0
Consultant neurologist, headache expert, historian of medicine, dog walker
Retired geriatrician, now working in human rights medicine & med ed; EBM; patient-centred care; equity & justice; polycurious & usually optimistic.
Refugee from Twitter (@Laconic_doc)!
Londoner, mother of two, consultant around questions of health, care, community, influence and impact (previously CEO Richmond Group of Charities and National Voices). Head and heart. 🐈⬛ 🪴 ☕️ 🇪🇺 🌳
100% health data nerd & OG swiftie. PhD Oxford Internet Institute. Previously Director of Policy Oxford Bennett Institute for Applied Data Science. Currently postdoctoral research associate Yale Digital Ethics Center.
ED Research Registrar (PGY8) at Royal Perth Hospital | Affiliate Researcher at Monash University | Major trauma & EM research. Husband🏳️🌈🇮🇪🇬🇧 views mine
Retired academic surgeon. PGY-thirtysomething. Surprisingly well behaved. Full-time dog servant. She/her. Surgeons can be female. So why can't (US) presidents? 🇨🇦-🇺🇸
#MedSky #SurgSky #MedEd #ILookLikeaSurgeon #Womeninmedicine #EndGunViolence
Expert by experience in healthcare management & policy, Chair National Voices, Trustee RVS, NED PHIN. Also cook, wine drinker, reader, gardener, walker, armchair art critic.
leading monthly multi-specialty journal for hospital doctors and other healthcare workers.
Link: https://magonlinelibrary.com/journal/hmed
Email:lydia@bjhmhealth.com
research manager, change manager, knowledge broker, compulsive fixer-of-things
Addressing #remoteandrural #coastal health issues. Associate Medical Director. Doctor. Anaesthetist. Darzi Fellow Alumnus. Once played cricket for Germany. All views my own
Elderly woman who refuses to behave like a granny Retired NHS librarian, OU graduate
Trying to cut the knowledge translation window down from over 10 years to less than 1 year with the power of social media.
Remember to be skeptical of anything you learn, even if you heard it on the Skeptics’ Guide to Emergency Medicine.
www.TheSGEM.com
West Midlands based salaried GP. Undifferentiated illness and symptom sorter.
Healthy Ageing Radio presenter, Amateur photographer, Explorer and Geriatrician in Bunbury WA 🇦🇺❤️😊👍🏽
I am a GP, wife and mum. I desperately want to see proper funding for our amazing NHS
Immediate Past President, Society for Acute Medicine (SAM)
Assoc Prof @Cambridge/ Director VPD HLRI Clin Res Facility/ expert faultitasker/ trades in barely informed science opinions/ views are personal
Epidemiologist with an interest in causal inference methods at @universityofleeds.bsky.social.
Check out my Intro to Causal Inference Course: https://www.causal.training/
#Epidemiology, #EpiSky, #CausalInference, #CausalSky, #AcademicSky
Respiratory and Sleep Medicine Hon Consultant Royal Brompton Hospital. Emeritus Professor NHLI Imperial College, London. Harveian Librarian Royal Coll Physicians. Supports Samaritans