Shmeta-analysis.
05.06.2025 18:06 — 👍 2 🔁 1 💬 1 📌 0
Post-treatment discontinuation eGFR trajectory is somewhat reassuring. No?
05.06.2025 16:08 — 👍 1 🔁 0 💬 1 📌 0
I think it is a positive first step, but whether there is a convincing evidence of an additive effect of combination therapy requires proof in an outcome study.
For now, combination therapy has won the bragging rights, but I would not go so far as to proclaim this is a practice-changing trial.
05.06.2025 15:47 — 👍 5 🔁 1 💬 1 📌 1
Is there a dose-response or a threshold relationship with UACR reduction and clinical outcome benefit? In other words, will a >50% reduction translate into a greater kidney or CV benefit than >30% reduction?
05.06.2025 14:59 — 👍 3 🔁 0 💬 1 📌 0
Hyperkalemia on combo vs nsMRA: RR 0.82, 95% CI 0.50-1.36
No clearcut evidence that hyperkalemia risk is mitigated by combining sglt2i with nsMRA (? Inadequate power/Sample Size)
05.06.2025 14:31 — 👍 4 🔁 1 💬 1 📌 0

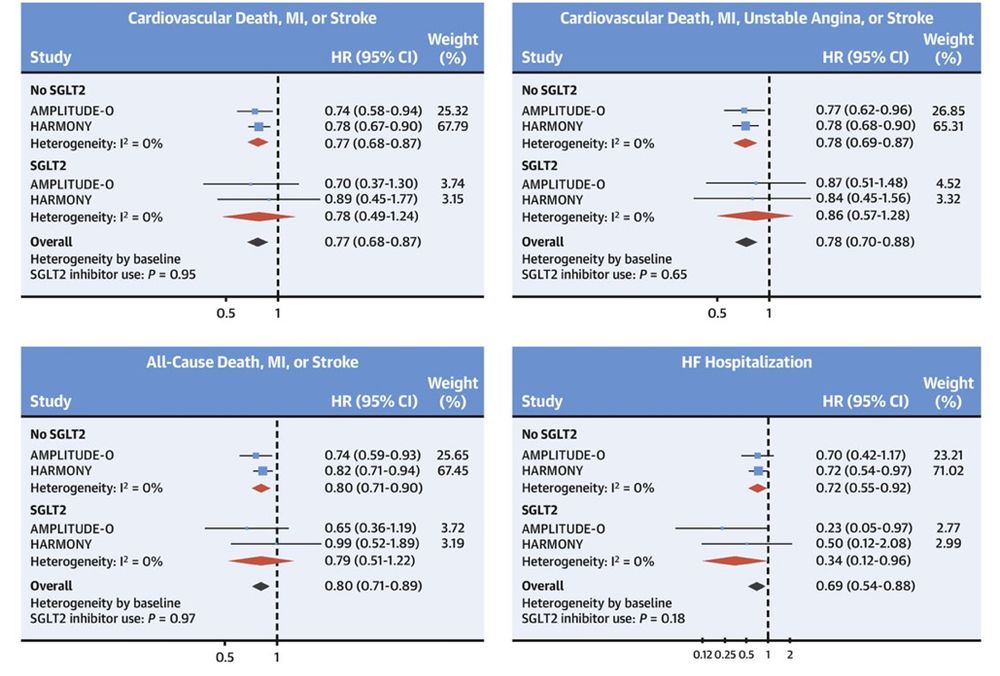
No 'additive' cardioprotective effect of GLP-1RA on background use of SGLT2i in HARMONY, AMPLITUDE-O and most recently SOUL.
Cardioprotective effects of GLP-1RA are 'independent' of SGLT2i
ahajournals.org/doi/epdf/10.11…
10.1016/j.jacc.2023.05.048
02.04.2025 22:25 — 👍 5 🔁 0 💬 1 📌 0
Pragmatic trials like comparative effectiveness studies require realistically ‘sober’ assumptions to account for the issues you stated.
Lipid hypothesis lingered on for several decades until LDL-C lowering was proven to reduce CV risk. Analogy applies to INOCA/ANOCA/MINOCA. Need novel targeted Rxs.
30.03.2025 23:20 — 👍 1 🔁 0 💬 1 📌 0
95% CI is compatible with a 6% benefit (clinically trivial) to 37% harm (clinically important). If CI contained a clinically important benefit, say HR of 0.80 or a more plausible HR of 0.85 to 0.90, but CI was wide spanning across HR of 1, then an inference of inconclusive result would be justified.
30.03.2025 23:16 — 👍 1 🔁 0 💬 1 📌 0
Trial powered for a HR of 0.80 which was excluded by the 95% CI.
Is it still a null outcome?
29.03.2025 15:03 — 👍 1 🔁 0 💬 1 📌 0
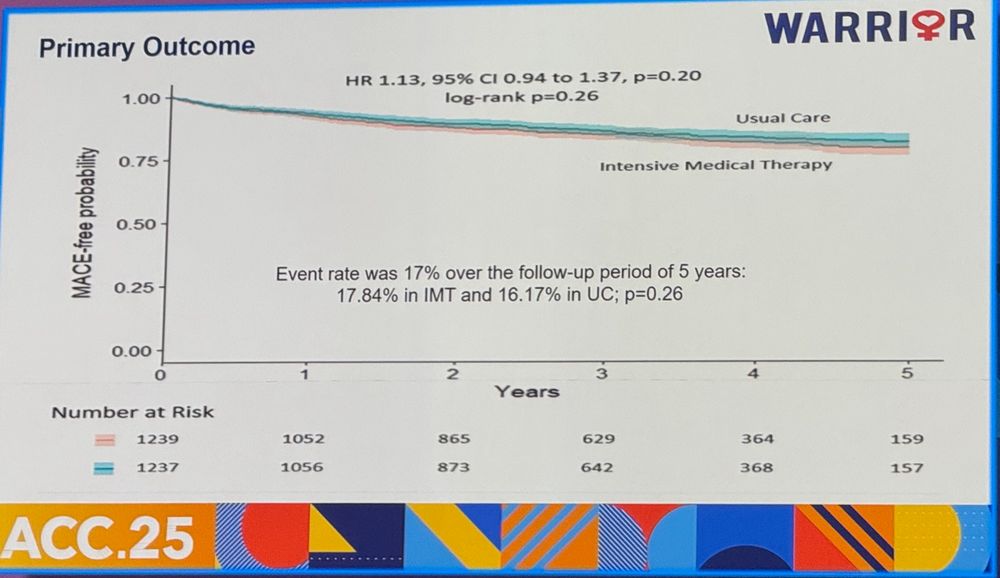
Warrior trial PEP result shown below.
Is this a NULL trial or a NEGATIVE trial?
Trial powered for HR 0.80 which was excluded by 95% CI
How many null or negative PRAGMATIC trials before we seriously consider/scrutinize the utility of such trials?
29.03.2025 15:02 — 👍 3 🔁 0 💬 2 📌 0
Are ORBITA trials practice-changing?
Very proud of this work with @kaulcsmc.bsky.social just published in Progress in Cardiovascular Diseases
Are ORBITA trials practice-changing?
We discuss whether the enthousiasm of some after ORBITA-2 is really justified.
www.sciencedirect.com/science/arti...
#medsky
#cardiosky
16.03.2025 20:10 — 👍 6 🔁 2 💬 0 📌 0
Are the Device Approval Standards Lax? JACC Cardiovasc Interv. 2025 Feb 10;18(3):380-384. doi: 10.1016/j.jcin.2024.08.037. PMID: 39939040.
Device Approval in the United States: The FDA Is on Target. JACC Cardiovasc Interv. 2025 Feb 10;18(3):385-387. doi: 10.1016/j.jcin.2024.10.044. PMID: 39939041.
16.02.2025 22:07 — 👍 0 🔁 0 💬 0 📌 0
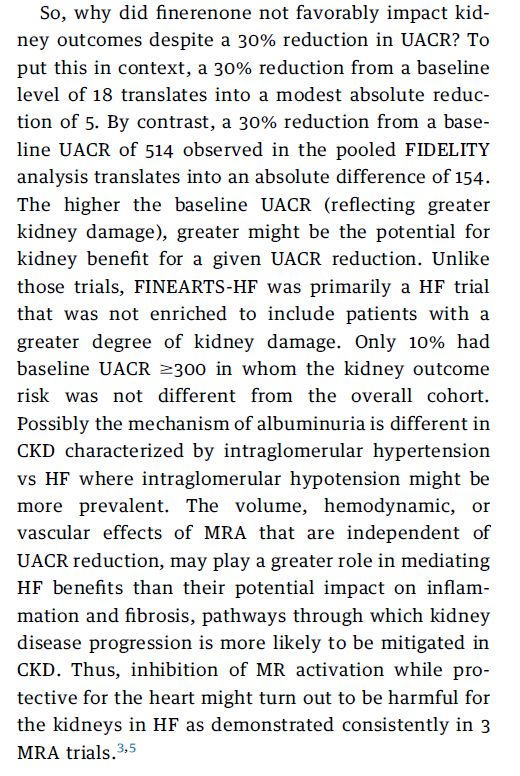
So, why did finerenone not favorably impact kidney
outcomes despite a 30% reduction in UACR? To
put this in context, a 30% reduction from a baseline
level of 18 translates into a modest absolute reduction
of 5. By contrast, a 30% reduction from a baseline
UACR of 514 observed in the pooled FIDELITY
analysis translates into an absolute difference of 154.
The higher the baseline UACR (reflecting greater
kidney damage), greater might be the potential for
kidney benefit for a given UACR reduction. Unlike
those trials, FINEARTS-HF was primarily a HF trial
that was not enriched to include patients with a
greater degree of kidney damage. Only 10% had
baseline UACR $300 in whom the kidney outcome
risk was not different from the overall cohort.
Possibly the mechanism of albuminuria is different in
CKD characterized by intraglomerular hypertension
vs HF where intraglomerular hypotension might be
more prevalent. The volume, hemodynamic, or
vascular effects of MRA that are independent of
UACR reduction, may play a greater role in mediating
HF benefits than their potential impact on inflammation
and fibrosis, pathways through which kidney
disease progression is more likely to be mitigated in
CKD. Thus, inhibition of MR activation while protective
for the heart might turn out to be harmful for
the kidneys in HF as demonstrated consistently in 3
MRA trials.3,5
Editorial on the renal results of FINEARTS HF in @jaccjournals.bsky.social from @kaulcsmc.bsky.social and moi
Free link:
authors.elsevier.com/a/1kQ%7Ec2d9...
#NephSky #CardioSky #Finerenone
13.01.2025 16:10 — 👍 15 🔁 6 💬 0 📌 0
Imagine if I excluded centers in a multicenter trial of SAVR vs TAVR where TAVR outperformed SAVR, I could show that SAVR was superior to TAVR in high-risk patients with AS (PARTNER-1A).
19.12.2024 19:48 — 👍 6 🔁 2 💬 2 📌 0
Should Heart Failure Trials routinely report on all-cause hospitalizations?
Should clinicians, guidelines & payers favor interventions that favorably impact cause-specific & all-cause outcomes?
jamanetwork.com/journals/jaman…
jamanetwork.com/journals/jaman
27.11.2024 17:19 — 👍 9 🔁 1 💬 1 📌 0
Who are the optimal candidates for acoramidis therapy?
When should it be considered first-line therapy?
Does the proposed cost provide value?
23.11.2024 01:42 — 👍 6 🔁 0 💬 1 📌 0
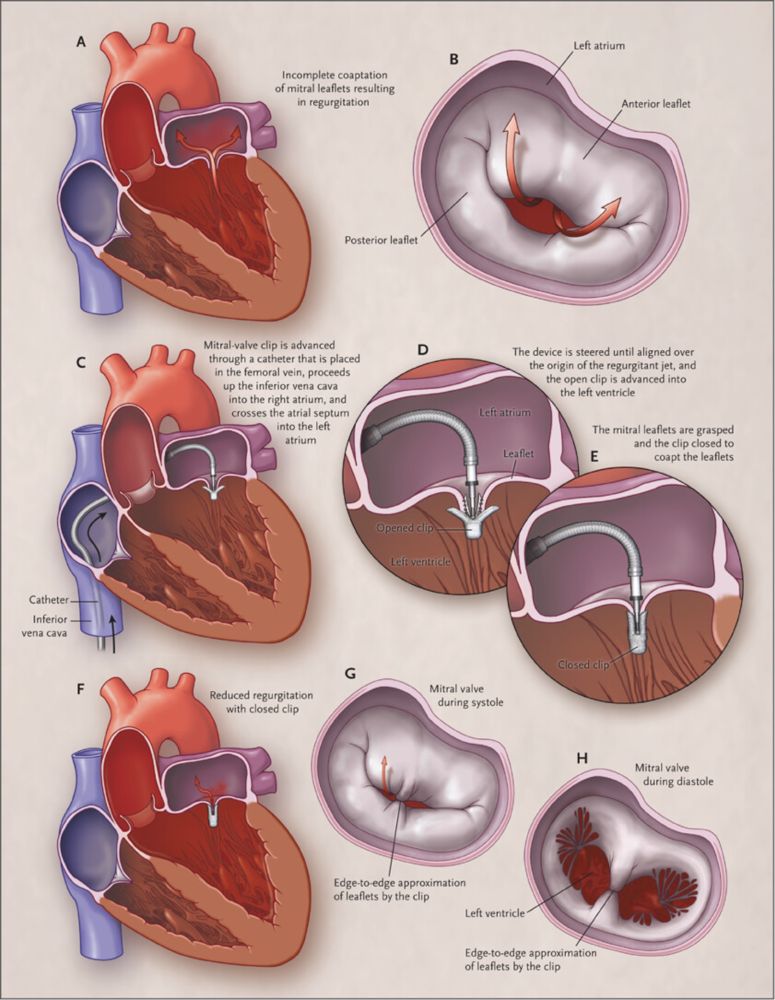
Percutaneous Repair or Surgery for Mitral Regurgitation | NEJM
Mitral-valve repair can be accomplished with an investigational procedure that involves the percutaneous implantation of a clip that grasps and approximates the edges of the mitral leaflets at the ...
NI margin in EVEREST II trial of MitraClip vs MV surgery for MR was 31% absolute difference, a margin through which one could drive 3 buses lined side by side.
Trial met NI despite the fact that HR excluded 1.0, i.e., MitraClip was INFERIOR to surgery, yet NONINFERIOR!
www.nejm.org/doi/full/10....
22.11.2024 02:33 — 👍 1 🔁 0 💬 0 📌 0
Even though the observed rates were lower than assumed (22%), had NI margin been fixed as risk ratio of 1.18 ([22+4]/22), the overall results would still have met NI as RR was 0.90, 0.77-1.05. An excellent example of how a NI trial should be designed and executed. Congrats to trial investigators.
22.11.2024 02:17 — 👍 1 🔁 1 💬 0 📌 0
So you are suggesting you need longer f/u and greater LDL and Lp(a) reduction, both of which favor PREVAIL. So what is the probability of success?
20.11.2024 21:20 — 👍 0 🔁 0 💬 1 📌 0
4/
Key Qs
What is probability of success with obicetrapib?
Why should obicetrapib succeed when 2 other CETPi did not?
Is absolute or relative LDL reduction key driver of benefit?
Is duration of treatment important?
Is LDL lowering with CETPi different from other LDL lowering Rx?
20.11.2024 05:42 — 👍 3 🔁 0 💬 0 📌 0
3/
PREVAIL(Obicetrapib), N=9541, F/U: ~4y
Mean LDL 103; LDL⬇️35-40%, Lp(a)⬇️45% (based on BROOKLYN)
PEP (4-MACE): Powered for 15-20% RRR
Recruitment completed; event-driven trial
Targeting higher baseline LDL & higher risk patients
20.11.2024 05:42 — 👍 4 🔁 0 💬 1 📌 0
2/
REVEAL (Anacetrapib), N=30,449, F/U: 4.1y
Mean LDL 61; LDL⬇️41%, Lp(a)⬇️25%
PEP (3-MACE): 10.8% vs 11.8%, HR 0.91, 0.85-0.97
Development halted (long half-life, modest Rx effect)
20.11.2024 05:42 — 👍 1 🔁 0 💬 1 📌 0
x.com
1/
Is LDL-C lowering by CETP inhibitor cardioprotective?
Brief history
ACCELERATE (Evacetrapib), N=12092, F/U: 28m
Mean LDL 81; LDL⬇️37%, Lp(a)⬇️22%
PEP (MACE-5): 12.9% vs 12.8% HR 1.01, 0.91-1.11
Trial stopped early due to futility
x.com/mdavidsonmd/...
20.11.2024 05:42 — 👍 5 🔁 1 💬 3 📌 0
Nonetheless, the clinical relevance of the favorable, but modest, MRI changes induced by Tirzepatide remain unclear.
19.11.2024 18:54 — 👍 1 🔁 0 💬 0 📌 0
What this graph tells us is that about 12% (R squared) of variability in LV mass can be explained by weight loss, thereby indicating that reduction in LV mass might be related to a possible direct cardiac effect or a paracrine effect,
possibly modulated via paracardiac adipocytes.
19.11.2024 18:49 — 👍 1 🔁 0 💬 1 📌 0
But need to know which criteria for CRNM bleed was driving it? There were 3 or 4 criteria specified? A visit to hospital or ER is more relevant than some other ones.
16.11.2024 21:16 — 👍 0 🔁 0 💬 1 📌 0
7/
So, what to make of a trial with 50% lower events than expected (sum total of 85 events over 3y in a trial enrolling 1600 patients), lots of missing data, & biased choice of safety outcome?
Enthusiasts of LAAC will celebrate 'win', but should clinicians & payers join in?
16.11.2024 20:07 — 👍 8 🔁 1 💬 0 📌 0
6/
But wait, should safety outcome not have captured procedural bleeding which is⬆️with LAAC? Had ISTH major bleed outcome (including procedural bleeding) been used, superiority would not have been met, and hence the win criterion would not have been met, strictly speaking!
16.11.2024 20:07 — 👍 4 🔁 0 💬 2 📌 0
Cardiologist, ❤️🩹Expert in Women & Heart Disease, Prevention, Author 'Saving Women's Hearts’- Heals 💔 Past President of ASPC #earlyinterventionalist @CedarsSinai #queenofhearts #CVPrev
Science integrity consultant and crowdfunded volunteer, PhD.
Ex-Stanford University. Maddox Prize/Einstein F Award winner
NL/USA/SFO.
#ImageForensics
@MicrobiomDigest on X.
Blog: ScienceIntegrityDigest.com
Support me: https://www.patreon.com/elisabethbik
Cardiologist, Clinical Trialist McMasterU. Heart failure, Cardiometabolic Disease, Implementation Science. Editor Circulation.
Cardiologist and researcher, in cardiovascular magnetic resonance imaging, at the University of Minnesota
Mayo Clinic diabetes doc + researcher + care activist working for careful + kind care for all. Wrote Why We Revolt 🇵🇪 (posts reflect my views, not employer’s)
Cardio-oncology Fellow @MSKCC
Professor of Cardiology at University of Catania, Italy. Director Division of Cardiology at Policlinico Hospital, Catania. Editor-in-Chief of EuroIntervention.
Cardiologist, professor at Keck-USC; believer in science, evidence-based medicine, health care as a right, a single payer system, democracy, and tennis.
Medical journalist, writer, and bestselling author of The Leap Year Gene (of Kit McKinley) and The Quintland Sisters.
#FamilyMedicine, Clinical Informaticist, EBM & Bioethics enthusiast | Faculty AdventHealth Family Medicine Residency | UFMEDICINE alum
#cardiometabolic #prevention; Multimodality #cvimaging; Posts may be my opinions & are not medical advice; RT≠endorse
Formerly known as @JJHeart_Doc on the "bird" app.
Professor of Medicine, Harvard; Cardiologist, MGH; Chief Scientific Officer, Baim Institute; Deputy Editor, JACC. Team MD for the Boston Red Sox.
I used to be disgusted. Now I try to be amused.
UCSF Hospital Medicine Physician Scientist at SFGH. Think about evidence, clinical medicine, outcomes, health services, policy. https://hopelab.ucsf.edu/people/anil-makam-md
End stage critical care cardiology trainee | #POCUS research | #Echo | #CriticalCare | #Physiology | #Equity | #SDH | #Statistics | #Rstats | #MedSky | #CardioSky | #CCCSky | #emimcc 🇳🇴🇩🇰 Trondheim, Norway
Cardiac Electrophysiologist at Reliant Medical Group and Cardiology Fellowship Associate Program Director
Husband, dog dad, musician, technology enthusiast
#EPeeps #CardioSky #MedSky
(Thoughts + posts are my own)
Burt Cohen, editor of the web's most extensive independent resource on stents & angioplasty for cardiologists & patients since 1997. #AngioHistory #BeforeGoogle #CardioSky
www.rickyturgeon.com
Cardiovascular pharmacist & Assistant Professor at UBC Faculty of Pharmaceutical Sciences.
EBM & shared decision making enthusiast, all-around nerd.
Heart Function Cardiologist, ❤️ 🇨🇦 Professor. Past Pres Federation of Medical Women of 🇨🇦 + Canadian HF Society. Clinical trialist. Everything Cardio-Kidney-Metabolic. #cardiosky #medsky
Cardiologist, Hypertension Specialist, Gardener, Director of Hypertension Section & AHA Comprehensive Hypertension Center @UTSW
Cardiologist health services researcher, editor, second luckiest man alive...