A meta-analysis of 5 contemporary trials found no improvement in outcomes with beta blocker therapy after myocardial infarction with normal EF (≥50%)
21.11.2025 16:12 — 👍 0 🔁 1 💬 1 📌 0
Conservative dialysis strategy shows promise for AKI-D
The LIBERATE-D trial found that this approach led to better renal recovery at discharge vs thrice-weekly dialysis (64% vs 50%)
Although adjusted CIs were nonsignificant and deaths were numerically higher
20.11.2025 20:14 — 👍 0 🔁 1 💬 1 📌 0
ICIs for NSCLC illustrates caution in broadening trial eligibility
In ECOG 0-1, trials show overall survival gain (65% vs 50% alive at 18 mos w/ chemo)
In ECOG 2+, excluded in trials & typical of hospitalized adults, survival is just ~4 mos
x.com/EvidenceRounds...
09.11.2025 16:25 — 👍 0 🔁 1 💬 1 📌 0
Many FDA-approved drugs receive indications broader than pivotal clinical trials, most notably for patient fitness
While broader labels can extend access, absolute benefits may be smaller or absent altogether, especially for sicker & more impaired hospitalized patients
08.11.2025 17:54 — 👍 1 🔁 1 💬 1 📌 0
The rise in early-onset cancer in the US, including colon cancer, is less an epidemic of disease & more an epidemic of diagnosis
The lack of a substantial rise in deaths, despite significant rising incidence strongly suggests increased diagnostic scrutiny & overdiagnosis
05.11.2025 15:35 — 👍 0 🔁 1 💬 1 📌 0
Routine use of gabapentin for postoperative pain is not supported by evidence
In a large multicenter double-blind RCT of patients undergoing major surgery, gabapentin did NOT improve pain, opioid use, length of stay, or quality of life
confirms a prior meta-analysis
30.10.2025 15:01 — 👍 0 🔁 1 💬 1 📌 0
Following the topline SNAP trial results, a new multicenter trial found cefazolin noninferior to cloxacillin for MSSA bacteremia, with fewer adverse events
Given its safety, convenience, and lower cost, cefazolin should be considered first-line therapy for MSSA bacteremia
28.10.2025 17:04 — 👍 0 🔁 1 💬 1 📌 0
You're gonna wanna follow this
Will be the single best way to have your finger on the pulse of what matters in hospital medicine and inpatient medicine more broadly
28.10.2025 17:17 — 👍 0 🔁 0 💬 0 📌 0
You misspelled clueless
03.10.2025 02:11 — 👍 0 🔁 0 💬 0 📌 0
This study seems riddled with selection and detection biases and I can't see how any knowledgeable expert could just take the results at face value and conclude a doubling of risk of long-covid with reinfection.
02.10.2025 04:56 — 👍 19 🔁 5 💬 2 📌 0
The Pros and Cons of the Latest FDA Actions on COVID Vaccines
In case you missed it, last week the FDA granted full approval for the Novavax COVID-19 vaccine. This vaccine, which uses a more traditional protein-plus-adjuvant strategy instead of the mRNA approach...
Recent FDA actions on Covid vaccines:
1. Novavax approved (👏)
2. Narrowed indications for all (pros and cons)
3. Called for clinical trials (👍)
No doubt we're relying too much on old data to inform clinical practice. Some thoughts on what we gain… and what we risk. blogs.jwatch.org/hiv-id-obser...
24.05.2025 11:30 — 👍 8 🔁 2 💬 7 📌 2
Agree for commercial insurance or Medicare
Too expensive within Medicaid
28.04.2025 02:43 — 👍 1 🔁 0 💬 0 📌 0
If there is one clinical driver of practice and it's not accounted for in any analysis I can't in any confidence trust the observational comparative effectiveness
Other than the rate of ODS is very very low which is most important part of evidence base
26.04.2025 18:32 — 👍 1 🔁 0 💬 0 📌 0
No, it does
It's just pseudo random but may correlate with other practice patterns and serve as a marker
26.04.2025 18:27 — 👍 0 🔁 0 💬 1 📌 0
FWIW I do fast correction for most
And if they live in low 120s from chronic badness I don't bother fixing it unless underlying issues fixable
26.04.2025 18:13 — 👍 1 🔁 0 💬 0 📌 0
Remains the sole clinical driver of speed
Rest is practice variation
Can't omit it and trust evidence at all
26.04.2025 18:11 — 👍 1 🔁 0 💬 2 📌 0
None of these adjust for chronicity
It's the major confounded here between an acute episodic thing vs chronic badness
26.04.2025 17:44 — 👍 1 🔁 0 💬 1 📌 0
Copied from my Twitter thread:
NOW WHAT?
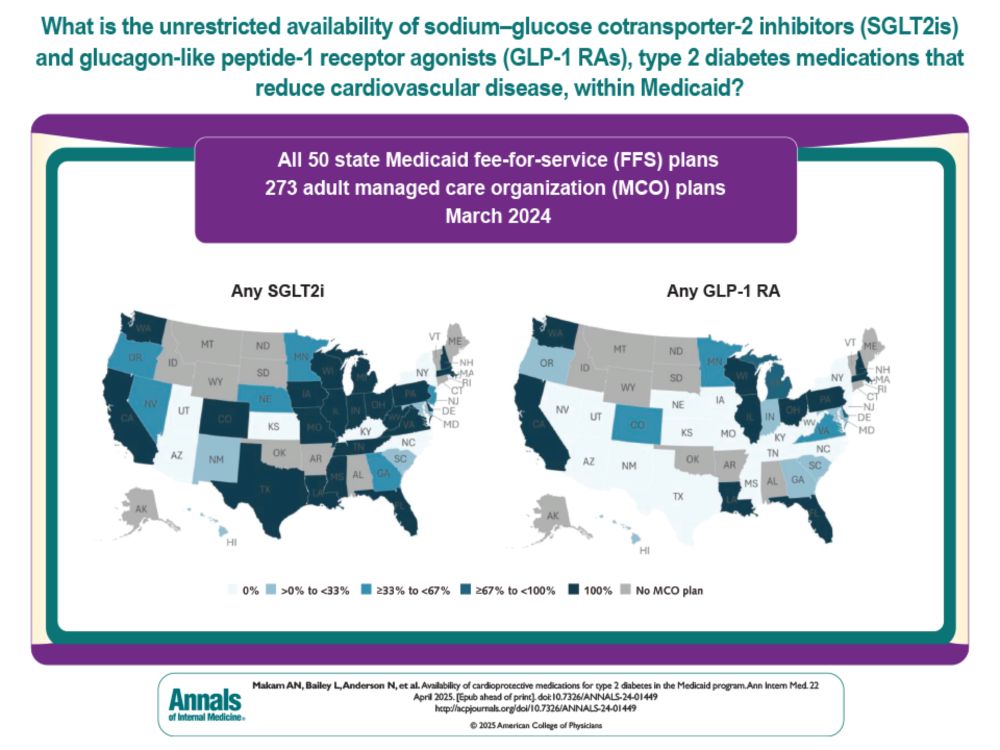
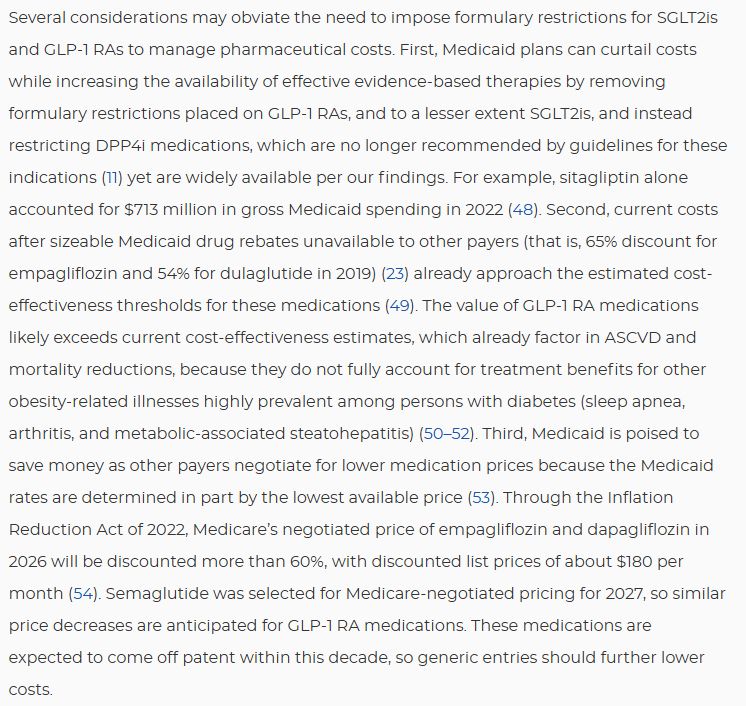
removing restrictions would improve access w/o step therapy (which makes no sense here) or prior auth
But $$$ is a real concern
Here is our pitch why may be less of an issue in Medicaid
AND
Restricting DPP4i instead of GLP/SGLT can offset some costs
23.04.2025 21:11 — 👍 0 🔁 1 💬 0 📌 0
Shared without comment.
19.03.2025 23:18 — 👍 923 🔁 174 💬 12 📌 7
x.com
This was inspired by an amazing study that I did a very popular Twitter thread on
x.com/AnilMakam/st...
05.02.2025 21:09 — 👍 0 🔁 0 💬 0 📌 0
Text in pictures
Link here
papers.ssrn.com/sol3/papers....
05.02.2025 21:09 — 👍 0 🔁 0 💬 1 📌 0
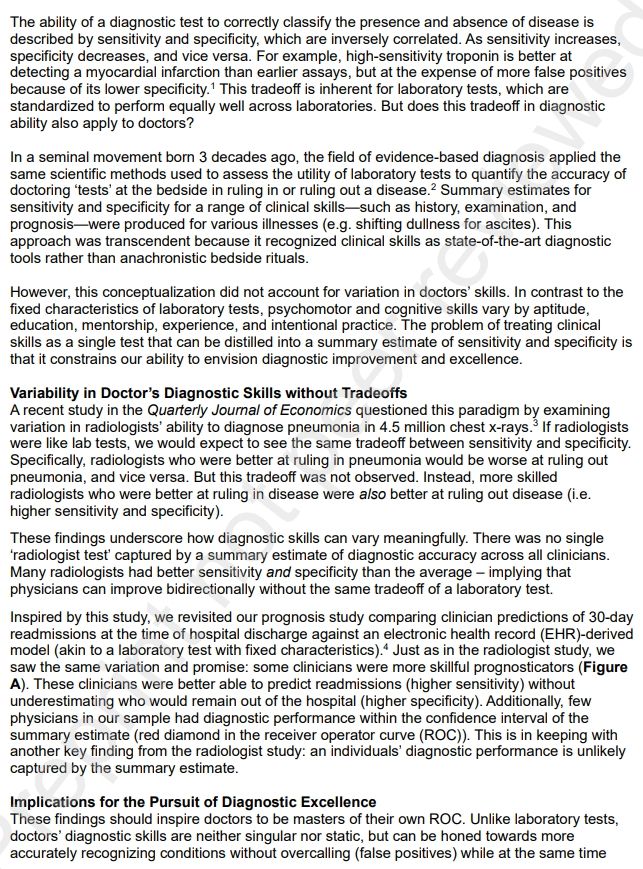
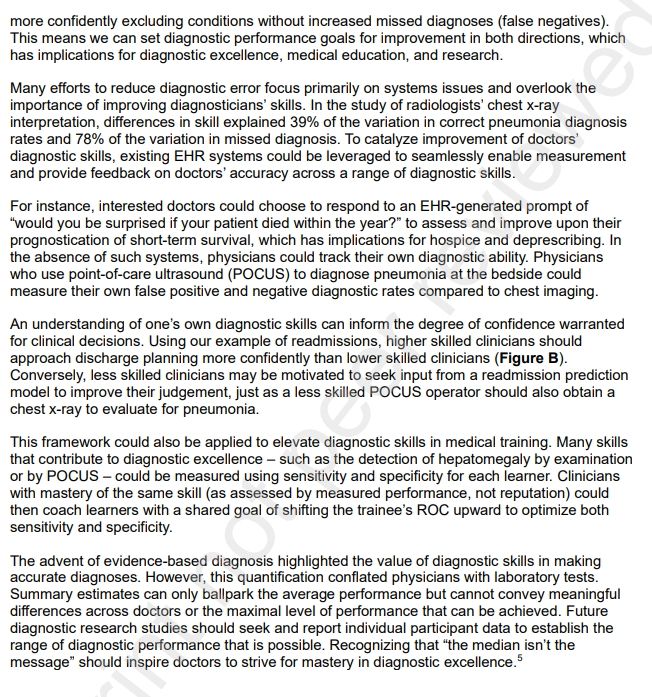
This matters because different skills translates to different probabilities for the same patient
05.02.2025 21:09 — 👍 0 🔁 0 💬 1 📌 0
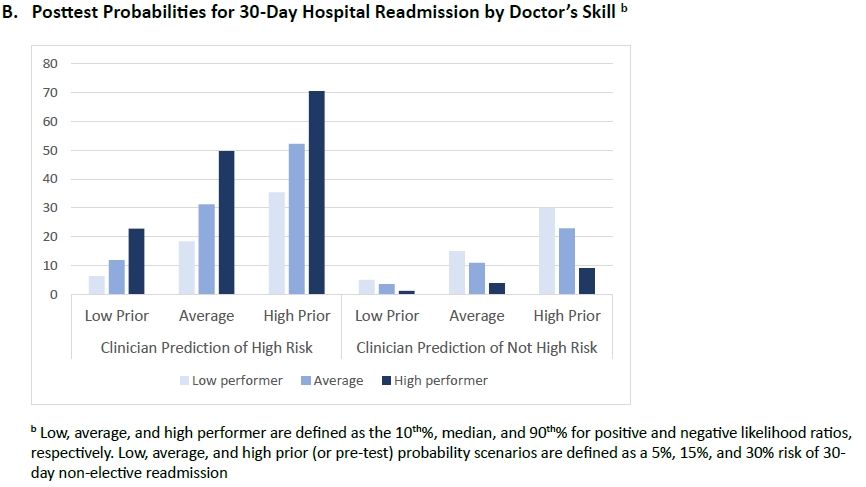
A key take home is that Doctors are unique diagnosticians
There is NO single 'doctor' with fixed abilities
What this means is that doctors can be the "master of their ROC" and strive for diagnostic excellence in both ruling in AND ruling out badness
05.02.2025 21:09 — 👍 0 🔁 0 💬 1 📌 0
I've been thinking more and more about evidence-based diagnosis
Penned this piece with Gurpreet & Oanh on the SSRN preprint server titled:
Striving for Diagnostic Excellence: "The Median Is Not the Message"
Tell me what you think
05.02.2025 21:09 — 👍 3 🔁 0 💬 1 📌 0
Agree. Not enjoyable so far. Place is great if you like echo chambers, especially ones that celebrate an assassination because of the industry. Thought the selling point was more sanity and compassion? Will lurk time to time to see if gets better, but find me at the other place
05.12.2024 06:14 — 👍 2 🔁 0 💬 2 📌 0
News you can use in hospital medicine
Medical literature is doubling rapidly, but knowledge isn't. Too many studies fail to answer the questions that matter most. We find and appraise the rare practice-changing evidence and cutting edge ideas.
Dermatologist | Health Services Researcher | Alum: @Morehouse @HarvardMed @MIT_HST @Kennedy_School | A naive EBM aficionado| Cancer researcher | Melanoma expert
Physician, Researcher, Advocate for the notion that an ounce of evidence is worth a pound of opinion. @brownpublichealth.bsky.social
My views are solely my own (who else would want them??)
Promoting improved patient care, research & education in primary care and general internal medicine. Join the conversation for #SGIM26!
Annals publishes content to inform medical professionals and society, advance standards of medical research, and improve the health of people worldwide.
Ezra Klein’s tweets, articles, clips and podcasts on Bluesky.
Premier peer-reviewed publication & the official journal for the Society of Hospital Medicine.
Physician, health policy analyst, executive at diagnostics company, writer, grammar obsessed.
Professor of medicine UCSF, GeriPal podcast, ePrognosis, JAGS, dad, husband, Ironman, Go Blue!
Internal Medicine specialist with a passion for inpatient education. Former Chair Board of Regents, American College of Physicians
General internist, health services and clinical researcher | Health, education, infrastructure, opportunity for all Americans | Bicycles | Opinions, own
Founded in 1942, the American Geriatrics Society (AGS) is a nationwide, not-for-profit society of geriatrics healthcare professionals dedicated to improving the health, independence, and quality of life of older people.
We are a comprehensive journal that matches the broad scope of general internal medicine (GIM) and we aim to promote advancements in clinical and health services research, medical education, and clinical practice in Internal Medicine.
Primary care physician/health policy research @yaleschoolofmed.bsky.social; @ncspyale.bsky.social; healthy skeptic; @jama.com deputy editor; open science: YODAProject @yalecrrit.bsky.social @medrxivpreprint.bsky.social
Primary care - health equity- cancer screening and prevention- health services research
Social Impact Leader. CEO @TexasTribune. Former @UnitedWay @TAAF @BeeckCenter | boards: @ConsumerReports @Internews Advisory Council @Pinterest @Comcast | love tennis, college basketball, volleyball and HGTV.
Health Economist and Editor in Chief with expertise in health economics and policy analysis
Stanford Visiting Scholar
Founder, AcademicHealth.com
Clin Prof of Medicine @GWSMHS & Assoc @JohnsHopkinsSPH
Former AAMC Executive
Walker of #Jasmine
A national newsroom that produces in-depth journalism about health issues; a core program of @KFF.org. Also publishes California Healthline.
The California Health Care Foundation (CHCF) is dedicated to advancing meaningful, measurable improvements in the way the health care delivery system provides care to the people of California.