Everyone thinks they are on the side of good.
24.07.2025 15:24 — 👍 0 🔁 0 💬 0 📌 0
Doing docs the other day. So many letters addressed to GPs that have not worked at my practice for 10+ years.
Would this be accepted in any other profession? 🤔
13.06.2025 13:39 — 👍 0 🔁 0 💬 0 📌 0
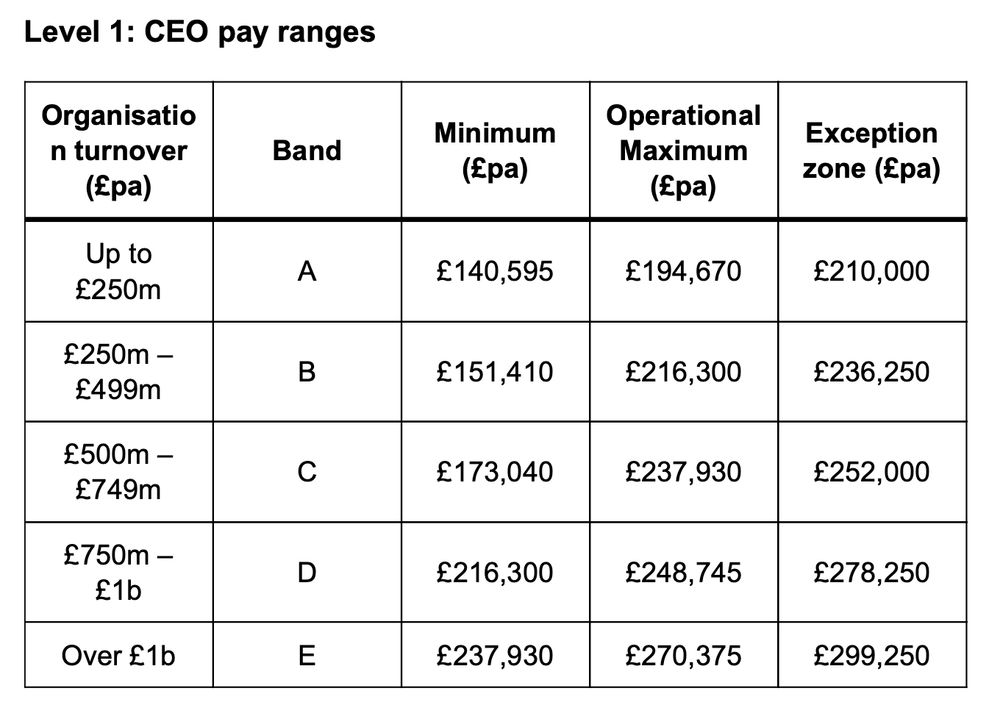
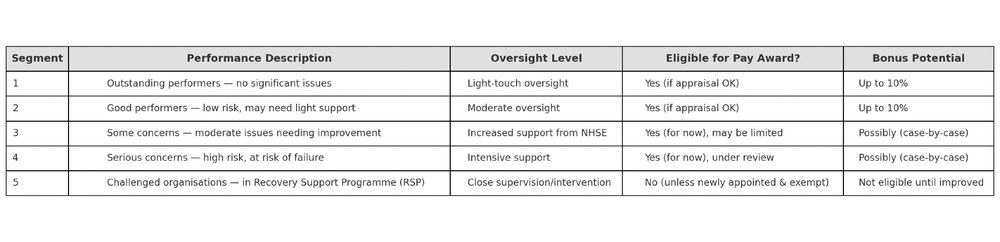
The new 2025 NHS very senior managers pay framework (yes it is called that) tries to shift that.
But it’s still layered on top of a structure that pays for scale, not sense.
Until that changes, the incentives won’t.
2/3
16.05.2025 10:45 — 👍 0 🔁 0 💬 1 📌 0
NHS Trust CEOs aren’t rewarded for collaboration.
They’re rewarded for control.
Bigger budget = bigger band = bigger pay.
Even if that means holding on when they should let go.
1/3
16.05.2025 10:45 — 👍 1 🔁 0 💬 1 📌 0
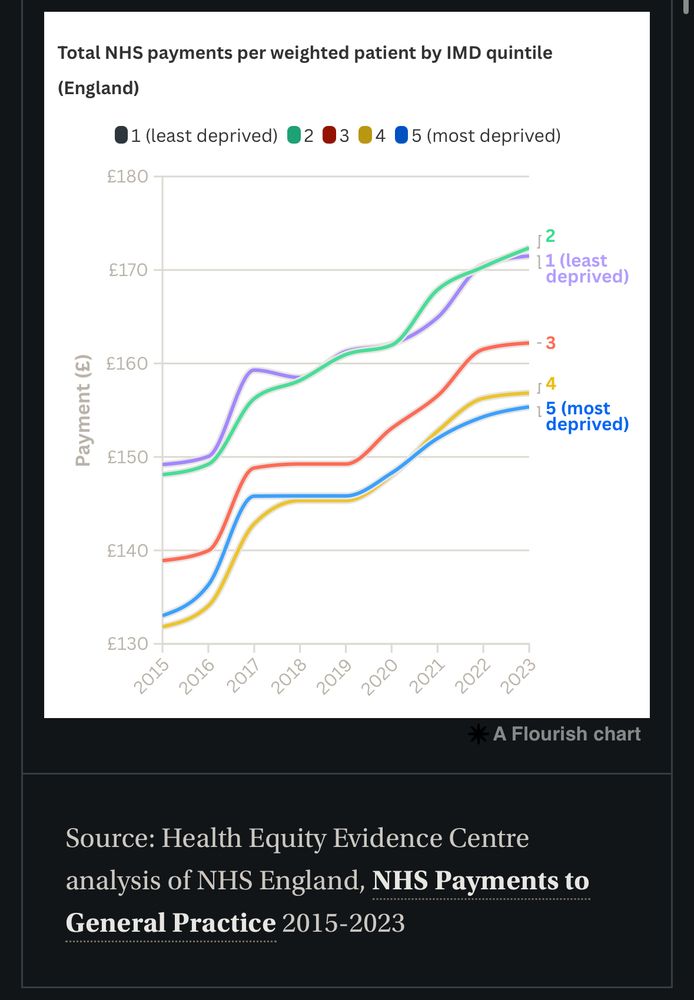
I spoke with someone from the voluntary sector while at an ICB event this week. He saw firsthand the gaps in our health and social fabric.
I explained how GP practices in poorer areas actually receive less funding than those in richer ones. His eyes widened. 😳He had no idea.
15.05.2025 13:45 — 👍 2 🔁 0 💬 1 📌 0
The Hills We Climb and the Winds We Forget
Headwinds, tailwinds and why progress rarely feels like progress in the NHS and in life.
The hills (that currently feel like mountains) will keep coming.
But remembering the wind at our backs might just make them a little easier to climb.
3/3
typeshare.co/anishkpatel/...
09.05.2025 13:44 — 👍 0 🔁 0 💬 0 📌 0
Psychologists call it the headwinds/tailwinds asymmetry.
We notice what holds us back more than what helps us forward.
A problem fixed is quickly forgotten.
We are experts as tracking hardship.
2/3
09.05.2025 13:44 — 👍 0 🔁 0 💬 1 📌 0
We talk a lot about what’s going wrong in the NHS. What’s broken. What’s missing.
That’s fair. There’s plenty.
But the danger is we only ever feel the climb.
1/3
09.05.2025 13:44 — 👍 0 🔁 0 💬 1 📌 0

What Gets Measured Gets Misunderstood
I’ve been looking at practice data for years, especially triage and call figures across GP surgeries
The NHS isn’t a machine. General practice isn’t a factory. When we treat it like one, we end up solving the wrong problems. AND create new ones.
3/3
typeshare.co/anishkpatel/...
08.05.2025 12:39 — 👍 1 🔁 0 💬 0 📌 0
Data strips out context. It becomes sterile, rigid, and dangerously clean. It flattens messy, human work into neat numbers that are easy to misinterpret and weaponise.
Especially when those at the coal face aren’t the ones holding the spreadsheets.
2/3
08.05.2025 12:39 — 👍 1 🔁 0 💬 1 📌 0
Everyone keeps saying better data will fix the NHS. But after years digging into triage and call stats across practices, I’ve realised the opposite is often true.
What gets measured gets misunderstood.
1/3
08.05.2025 12:39 — 👍 0 🔁 0 💬 1 📌 0
So we triage. We sort. We see those most in need.
And today, that means you must go elsewhere.
I am sorry. 😔
02.05.2025 07:06 — 👍 1 🔁 0 💬 0 📌 0
All I want to do is bring you in.
To sit you down.
To help you—the way we are trained to.
As a team, we handle most of what walks through our doors.
But there aren’t enough of us to go around.
02.05.2025 07:06 — 👍 1 🔁 0 💬 1 📌 0
All I can offer now is advice:
• Visit the local chemist, with their rigid list of conditions they’re allowed to treat, or
• Head to the urgent care centre, where you will be seen—but you may wait for hours.
02.05.2025 07:06 — 👍 1 🔁 0 💬 1 📌 0
I work through the list, one by one, trying to make the most of what we have to offer.
And now we return to you.
Everything has gone. No more appointments. The end of the road.
02.05.2025 07:06 — 👍 1 🔁 0 💬 1 📌 0
I pause over your request.
I come back to you—not because you’re unworthy of my time, but because I must ask:
Is there someone even more in need?
02.05.2025 07:06 — 👍 1 🔁 0 💬 1 📌 0
To the Patient I Had to Turn Away 🧵
I see you on my triage list, staring at me.
I see the worry etched across your words. I see the fear.
But I also hear the others calling out just as loudly.
02.05.2025 07:06 — 👍 2 🔁 1 💬 1 📌 0
I’ve always treated the patient record with a massive pinch of salt.
AI scribes are the great hope. But a practical coding ability with write back into the EPR is not quite there yet.
01.05.2025 13:10 — 👍 1 🔁 0 💬 0 📌 0
Massive bug bear of mine.
Ultimately though comes down to: “the working culture and conditions”.
- When you are taught how to use electronic patient record (EPR) by osmosis
- When people don’t realise how problem codes work, as they never been told
- When you don’t have time to clean things up
01.05.2025 13:10 — 👍 1 🔁 0 💬 1 📌 0
Burnout by Design
Burnout isn’t a flaw. It’s a feature of the system.
Every delay.
Every hoop.
Every added task with no time to do it.
It’s not a glitch.
It’s a structure that drains the people it relies on.
We don’t burn out by accident.
We burn out by design.
typeshare.co/anishkpatel/...
25.04.2025 07:46 — 👍 0 🔁 0 💬 0 📌 0
It should be the most meaningful job in the world.
You help people when they’re scared, broken, or lost.
But instead of feeling fulfilled, you feel empty.
This is what burnout in the NHS really feels like.
And it’s not just happening.
It’s being designed into the system.
25.04.2025 07:46 — 👍 1 🔁 0 💬 1 📌 0
YouTube video by Dr Anish K Patel
Richer Areas Get MORE Funding – Why It Matters & How It Happened
Trying something new – creating YouTube videos. Turns out talking to a camera is way harder than it looks, but I’m giving it a go. First up: how NHS GP funding is rigged against poorer areas. Let’s see how this goes… 🎥👇
youtu.be/D-oXS45gIbA
16.02.2025 20:02 — 👍 0 🔁 0 💬 0 📌 0
The real Q is: Will those in power fund a safe and sustainable general practice?
We’ll find out in the 10-year NHS plan
📊 The Gold Standard: 1 GP per 1,000 pts
📈 The need: 2,859 FTE GPs per year
🎓 The pipeline: 6,000 GP Regs per year by 2031
💰 The missing piece: Funding
[End]
07.02.2025 13:14 — 👍 0 🔁 0 💬 0 📌 0
A Choice
This can be fixed
If we commit to funding new GP posts, we can:
✅ Make sure practices can afford to hire GPs
✅ Improve retention by spreading workload fairly
✅ Stop the brain drain to other countries
This is not a fantasy. The numbers do work.
07.02.2025 13:14 — 👍 0 🔁 0 💬 1 📌 0
The Global Competition
GPs are in demand worldwide. Canada, Australia, and New Zealand offer better pay, better working conditions, and a better work-life balance.
We are already training many of the world’s GPs. Do we want to keep them, or export them?
07.02.2025 13:14 — 👍 0 🔁 0 💬 1 📌 0
Adding 1️⃣+2️⃣ = The Freezing of GP Posts
A dangerous trend is emerging: as GPs leave, many practices will freeze their positions. Not because they don’t need a replacement, but because they can’t afford to hire one while keeping the lights on.
07.02.2025 13:14 — 👍 1 🔁 0 💬 1 📌 0
2️⃣ Hiring: A Funding Crisis
Another problem has emerged: qualified GPs can’t find jobs. It sounds absurd—we need more GPs, yet practices can’t afford to hire them. It is a failure to fund GP posts.
07.02.2025 13:14 — 👍 1 🔁 0 💬 1 📌 0
Economist at the IFS working on health and social care, public spending and public sector productivity https://ifs.org.uk/people/max-warner
FY10 (GPST4 ACF) Birmingham UK.
Academia, Athletics and #MediCurious
#MedSky #GPSky
NHS General Hacktitioner GP, NHS IT, Software Dev
Everything Digital Health everythingdigitalhealth.com
RCPCH Digital Growth Charts https://growth.rcpch.ac.uk/
Freelance Health Tech and Discourse Forum syadmin https://bawmedical.co.uk/
GP, @RCGP Vice Chair, Research & Innovation lead @NHS_NELondon, @FSEM_UK sports medicine @QMUL . May your choices reflect your hopes, not your fears. Views: mine
GP, Cambridge | Associate Director, Health Equity Evidence Centre | Development Director, Cambridge City Foodbank | Co-lead, The Big GP Consultation | Former NMD's Clinical Fellow, NHS England
GP, educator and co-author of Fighting for the Soul of General Practice- the algorithm will see you now; and the series of linked podcasts on YouTube. I am currently editing a textbook on finding and creating meaning in healthcare, my main area of interest
From the experience of @stitches.today, we bring you the best papers in medicine, daily in your inbox - for free!
Subscribe 👉 www.stitches.today/medicine
Supporting GPs and their general practice teams to manage complexity and championing whole person healthcare.
Website: https://www.wisegp.co.uk
Newsletter sign-up: http://wisegp.co.uk/sign-up
GP. NIHR Academic Clinical Lecturer, CAPC, Bristol Uni.
Project lead www.gpevidence.org
RCGP Overdiagnosis Group, NICE GP Reference Panel, Assoc Editor DTB
Busy NHS Director of Primary Care in Devon. Occasional health and care commentator. Enthusiastic smallholder. Keen angler.
We want people to be able to share their experiences of health and care in ways which are safe, simple, and lead to learning and change.
Care Opinion CIC (non-profit) | https://www.careopinion.org.uk
We fund vital research into heart diseases, stroke and vascular dementia, and their risk factors like diabetes.
We’re the world's leading independent cancer charity dedicated to saving lives through research, influence and information.
linktr.ee/cr_uk
Patient Safety Learning is a charity and independent voice for improving patient safety.
🔗Our website: https://www.patientsafetylearning.org/
🔗the hub, our platform to share learning for patient safety: https://www.pslhub.org/
NHS Employers is the employers’ organisation for the NHS in England. We support workforce leaders and represent employers to develop a sustainable workforce and be the best employers they can be.
Part of @nhsconfed.org
🔗 www.nhsemployers.org
We are the world’s leading provider of professional protection for doctors and healthcare providers.
🔗 www.medicalprotection.org
We are an independent charitable organisation working to build a healthier UK.
www.health.org.uk
We are the membership organisation that brings together, supports and speaks for the whole healthcare system in England, Wales and Northern Ireland.
www.nhsconfed.org
We represent around 40,000 physicians worldwide - educating, improving and influencing for better health and care.