
 12.06.2025 21:11 —
👍 6
🔁 1
💬 1
📌 0
12.06.2025 21:11 —
👍 6
🔁 1
💬 1
📌 0
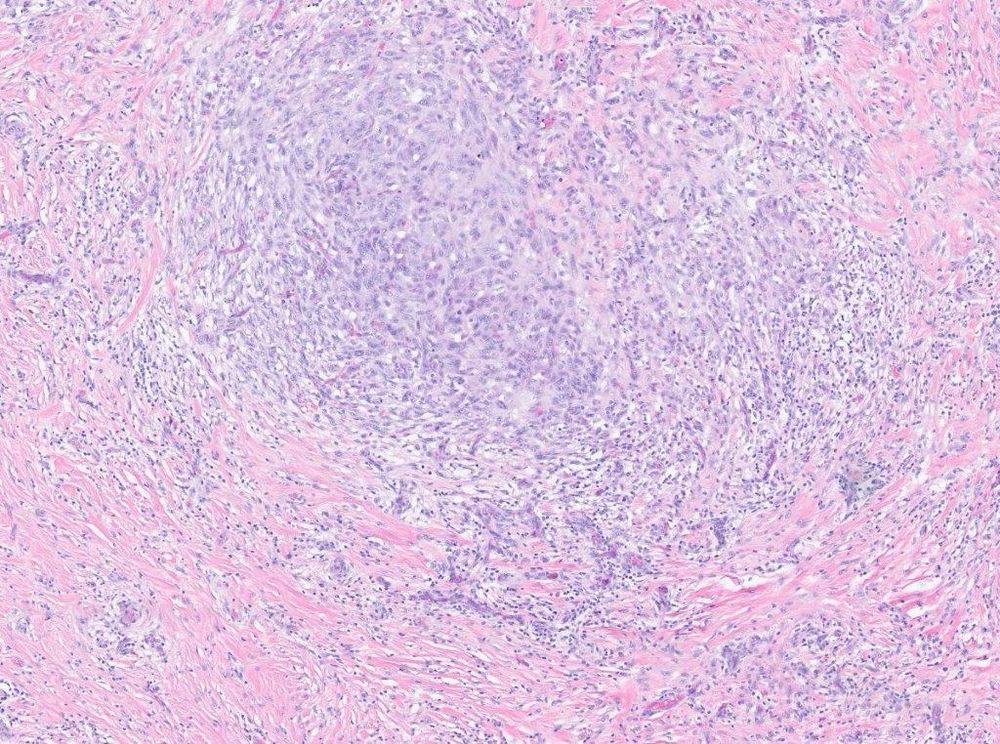
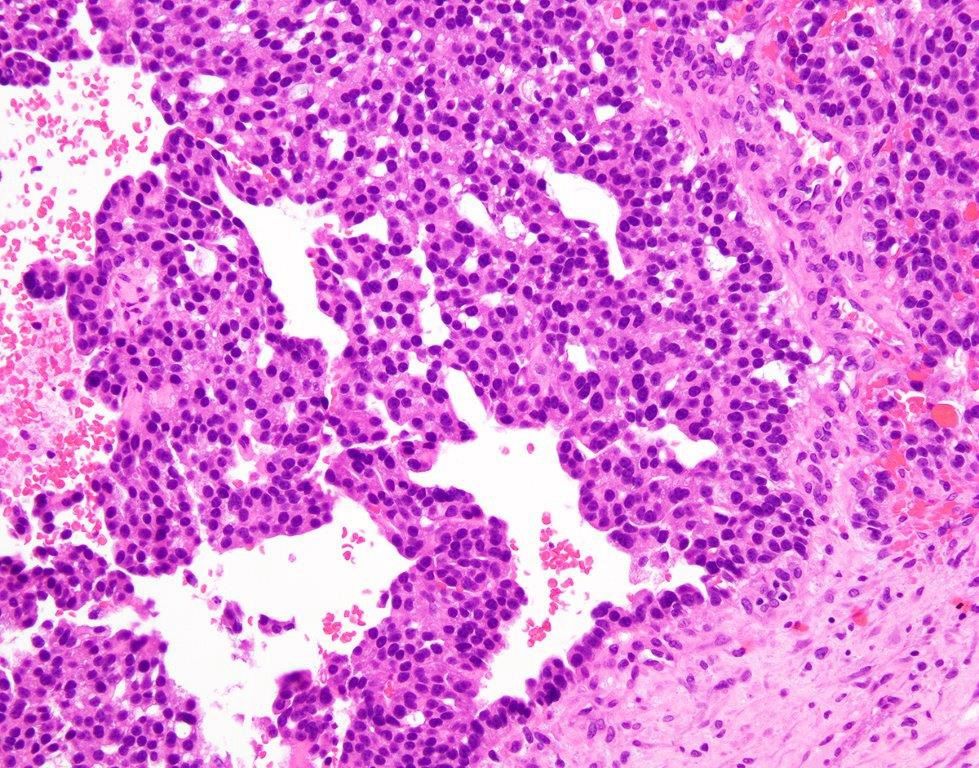
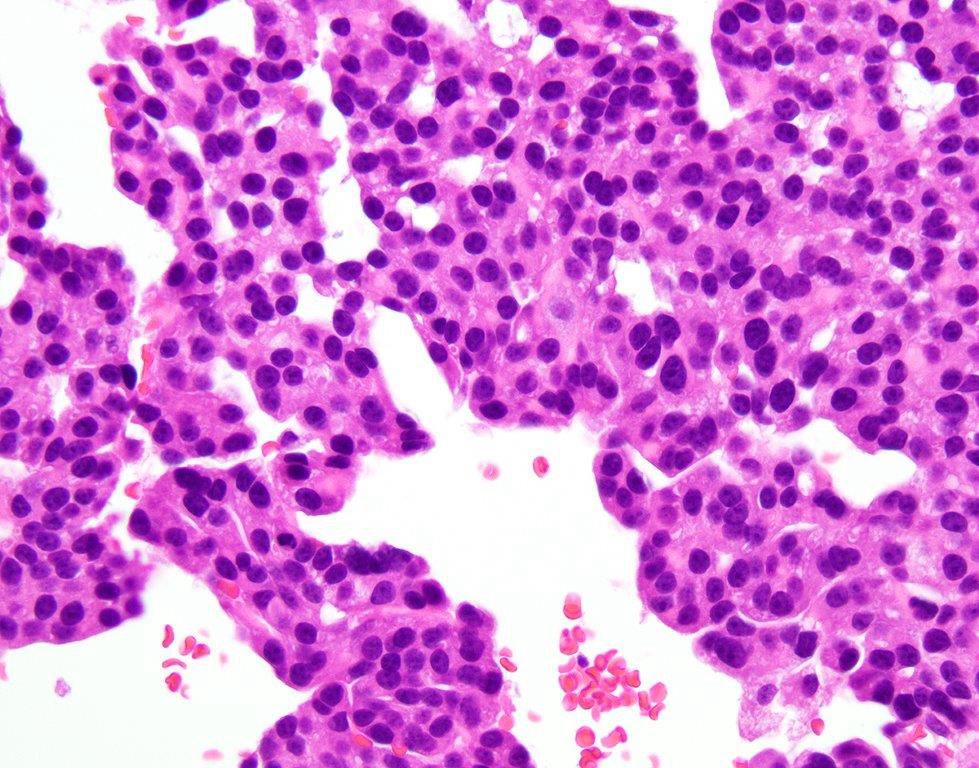
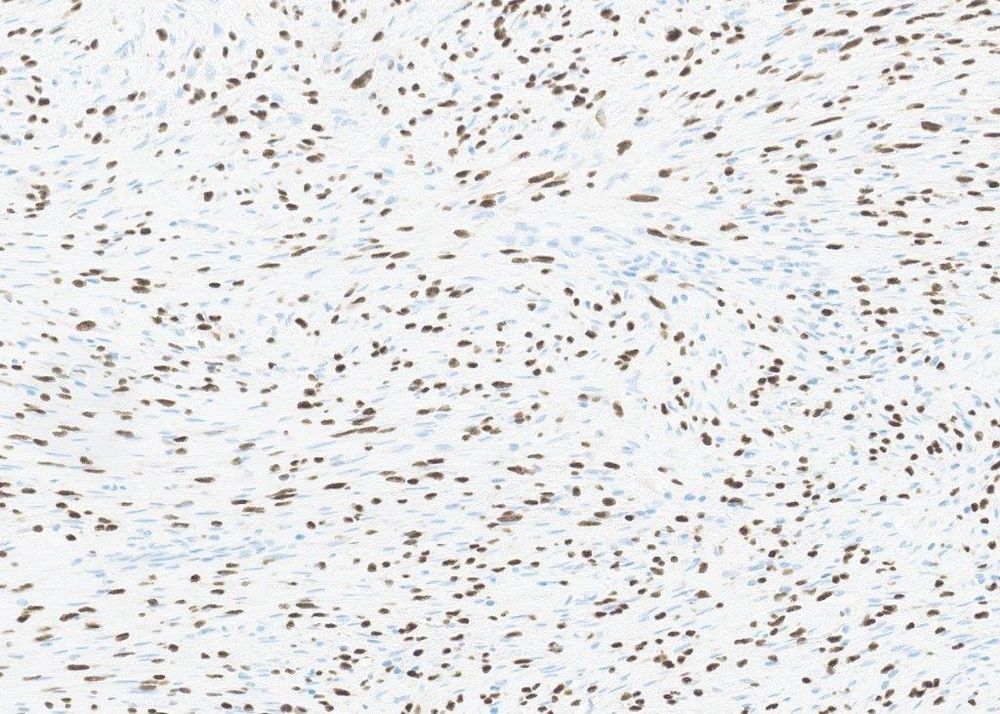
This is classic morphology for a GLI1 coamplified differentiated liposarcoma with perineurial-like whorls. So now the MDM2 amplification makes sense. The current tumor is showing essentially classical features of a GLI1 amplified soft tissue sarcoma. So the morphology/molecular explain each other.
12.06.2025 21:10 — 👍 5 🔁 1 💬 1 📌 0

Last 2
12.06.2025 21:06 — 👍 1 🔁 0 💬 1 📌 0


Well, it turned out he had a tumor in the same laryngeal location a few years ago, diagnosed as a “fibroinflammatory lesion with some features of IgG4 disease”.
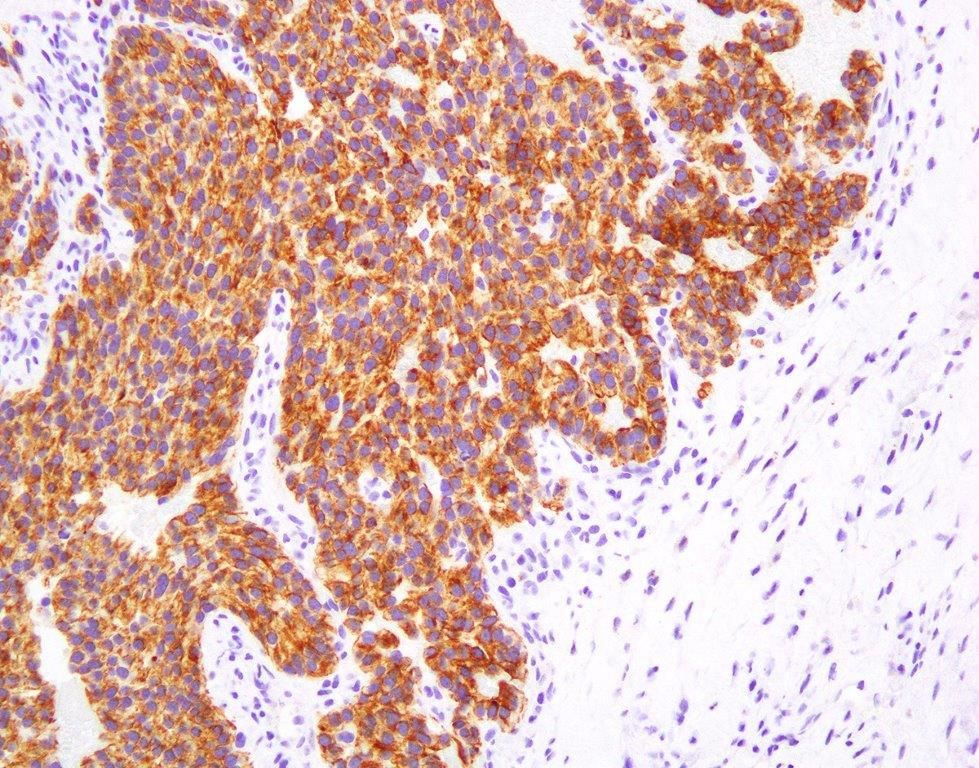
12.06.2025 21:06 — 👍 1 🔁 0 💬 1 📌 1A big panel of IHC was negative. For somewhat unclear reasons, MDM2 FISH was ordered and was amplified. Does this make any sense?
12.06.2025 21:03 — 👍 1 🔁 1 💬 1 📌 0

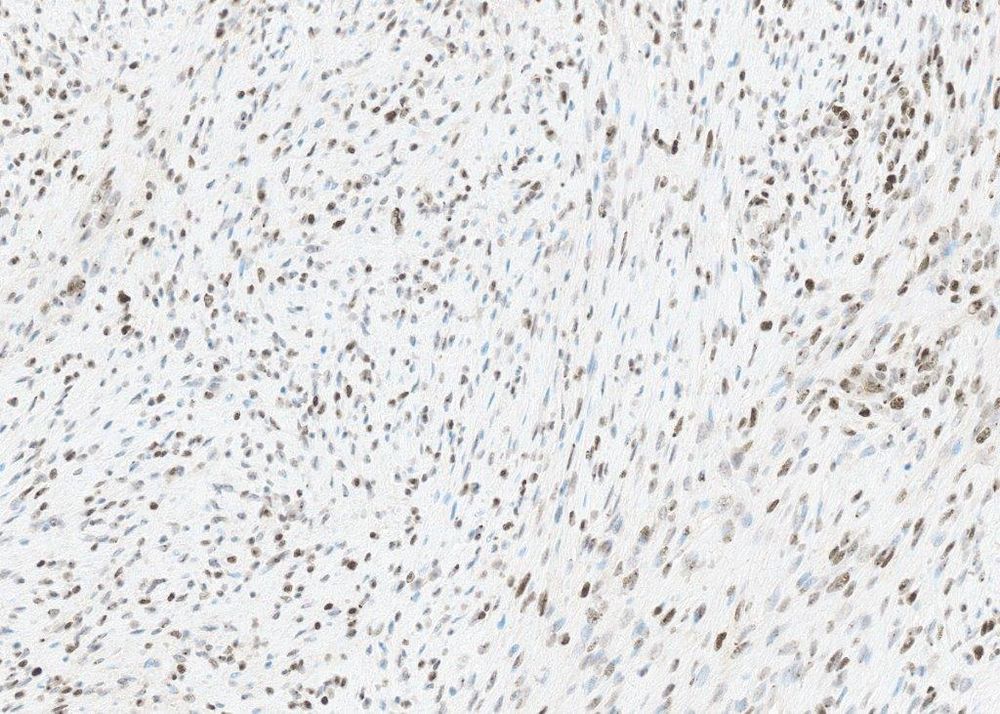
It’s also got some bland spindle cell areas.
12.06.2025 21:02 — 👍 1 🔁 1 💬 1 📌 0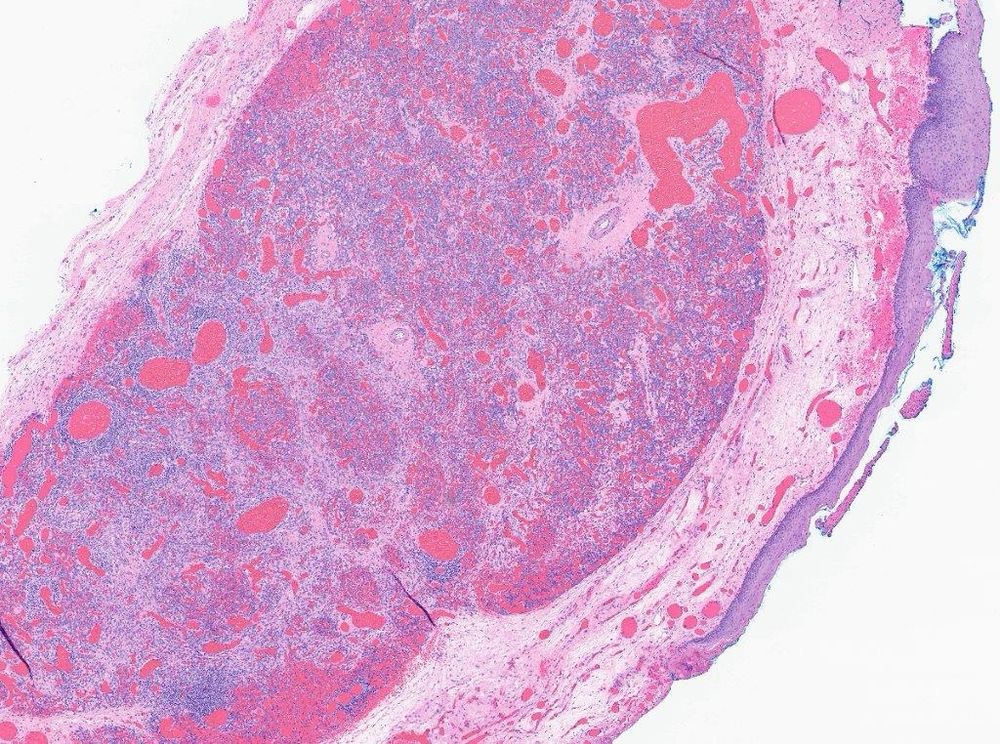
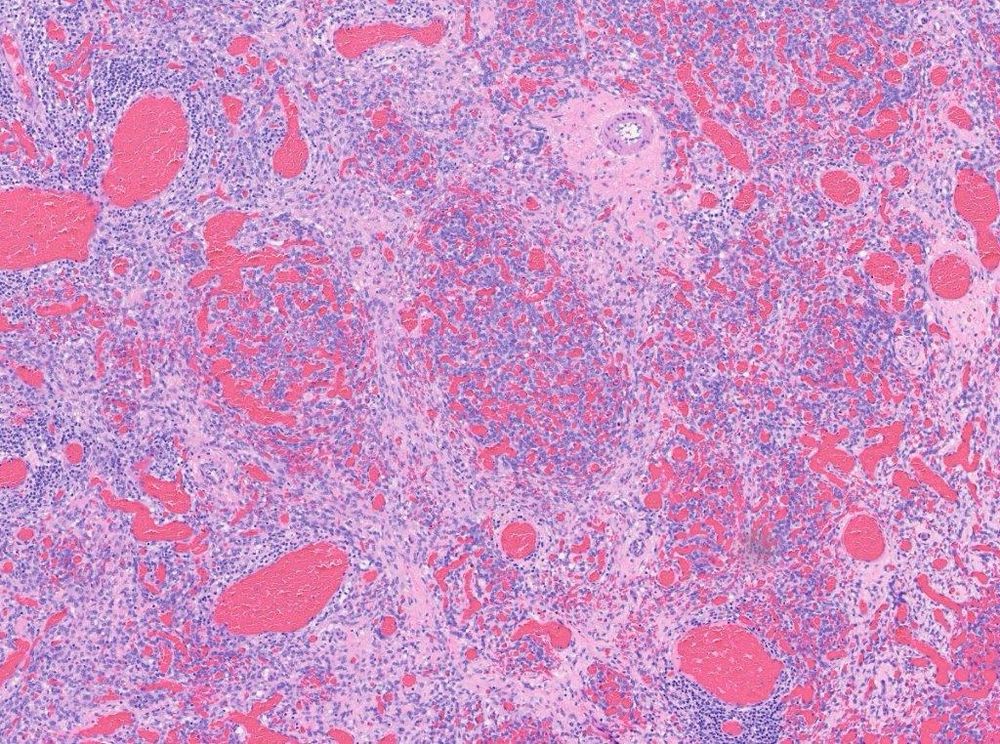
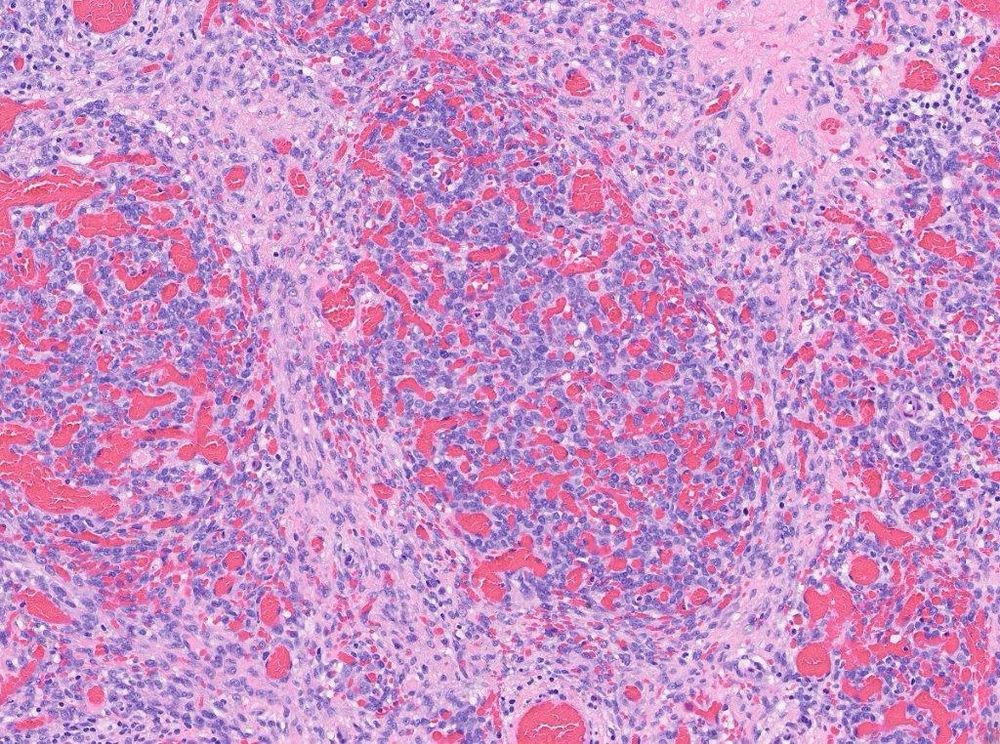
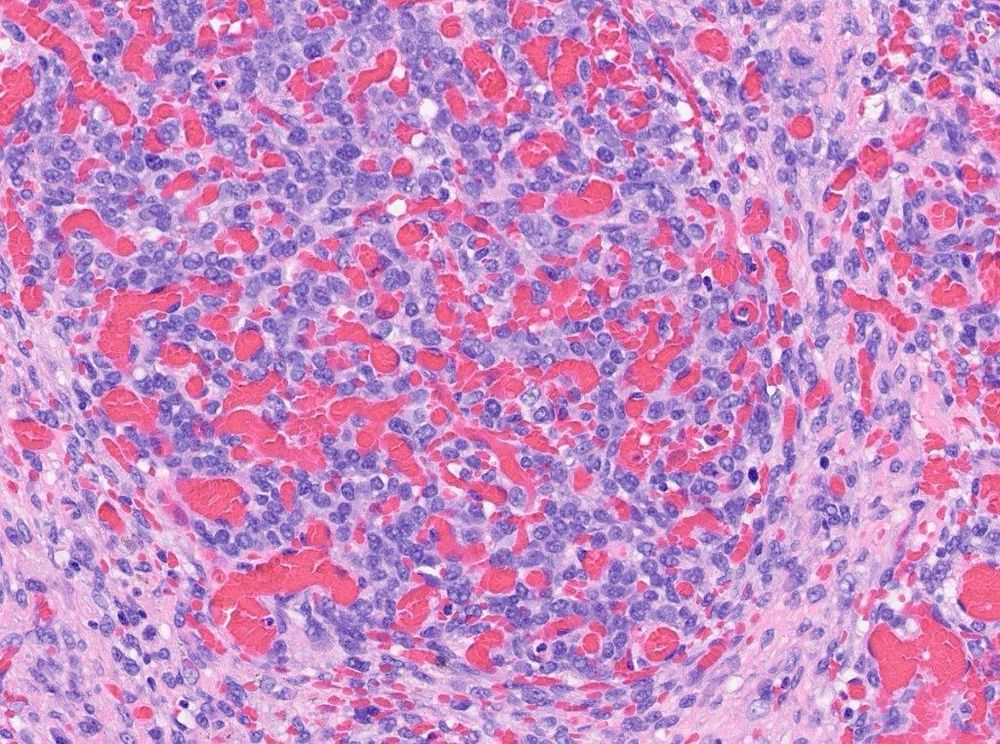
#PathSky Laryngeal mass, older adult male. Primitive, highly vascular round cell neoplasm for the most part.
12.06.2025 21:00 — 👍 9 🔁 6 💬 1 📌 0Epithelioid angiosarcoma with extensive intravascular growth. Obviously there must be a right sided primary. There’s supposed to be a liver mass.
05.06.2025 19:20 — 👍 6 🔁 1 💬 0 📌 0
CD20

CD31

CD34
Just because the ddx includes intravascular lymphoma (at one time known as “intravascular angioendothelioma”), the first pic is CD20. The others of course are CD31 and CD34.
05.06.2025 19:17 — 👍 3 🔁 1 💬 1 📌 0



#PathSky 53F with shortness of breath and “ground glass” pulmonary opacity. Not a hard dx, but a spectacular (if very unfortunate) case.
05.06.2025 19:14 — 👍 12 🔁 5 💬 1 📌 0
So- desmoid fibromatosis with bizarre cells and p53 mutant pattern- r/o Li-Fraumeni syndrome.
Happy Friday!
pubmed.ncbi.nlm.nih.gov/36908221/

P53

P53
There is a single case report of a desmoid occurring in a Li-Fraumeni patient, with identical morphology. p53 IHC done on this case shows a null/mutated pattern.
30.05.2025 17:35 — 👍 5 🔁 1 💬 1 📌 0



Fear not. It’s also got these really bizarre cells, all over the place. Those don’t belong in a desmoid! Not a desmoid? Or is there another explanation?
30.05.2025 17:33 — 👍 5 🔁 1 💬 1 📌 0



Beta-catenin
#PathSky Abdominal wall mass, middle aged woman. Women basically only get 3 abdominal wall tumors, so it’s got to be a desmoid, DFSP or endometriosis. Classic desmoid morphology, aberrant nuclear beta-catenin. I can hear the cries of “boring..”
30.05.2025 17:31 — 👍 9 🔁 3 💬 1 📌 0#PathSky Someone shared a chest wall Ewing sarcoma with me today, and I queried them about exactly what they were Askin. I should probably retire today.
23.05.2025 16:42 — 👍 6 🔁 0 💬 3 📌 1I wrote a complaint.
20.05.2025 21:42 — 👍 3 🔁 0 💬 1 📌 0
SS18-SSX

SSX c-terminus
Pics would be nice, right?
20.05.2025 21:33 — 👍 9 🔁 0 💬 1 📌 0
It’s diffusely positive for SS18-SSX fusion protein and SSX c-terminus antibody. Monophasic synovial sarcoma, with nuclear palisading. Yes, I’ve seen this before. No, not anywhere near this much. pubmed.ncbi.nlm.nih.gov/32141887/
20.05.2025 21:32 — 👍 7 🔁 1 💬 1 📌 0


#PathSky Middle aged woman, leg mass. It all looks like this. More nuclear palisading/ Verocay bodies than you’ve seen in your entire career. Nerve sheath? S100/Sox10 negative. LMS? Negative for all the muscle markers. Any other ideas?
20.05.2025 21:30 — 👍 13 🔁 5 💬 3 📌 0Oh, ok. Thx.
15.05.2025 23:13 — 👍 0 🔁 0 💬 0 📌 0?
15.05.2025 10:39 — 👍 0 🔁 0 💬 1 📌 0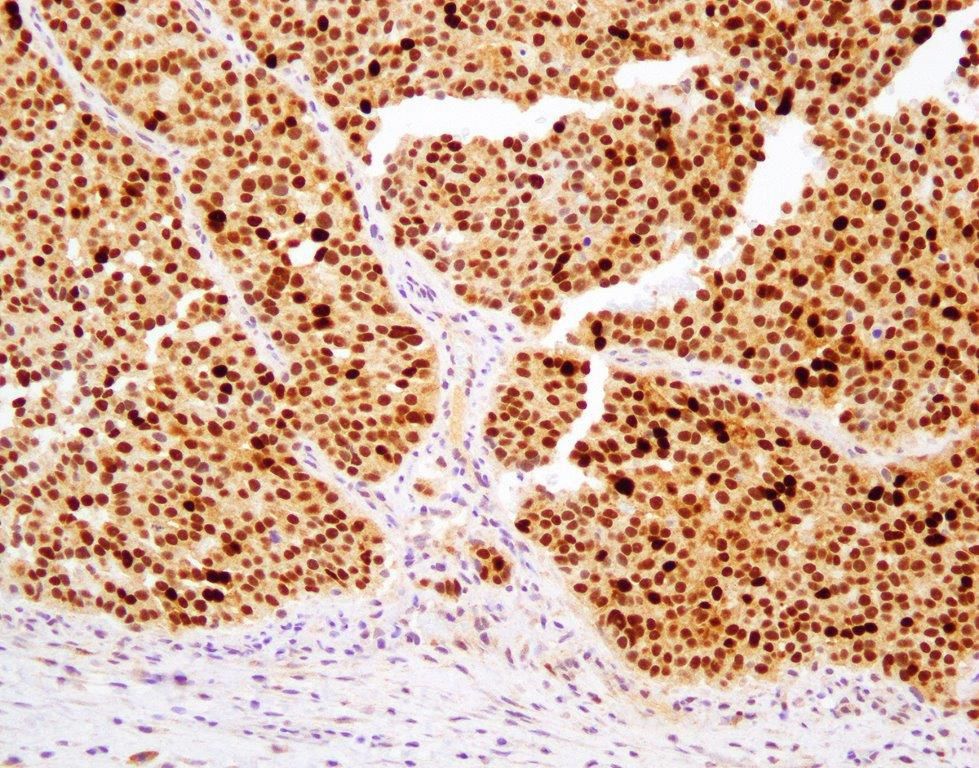
MDM2

Oops, I forgot the MDM2 photo.
14.05.2025 15:29 — 👍 7 🔁 0 💬 1 📌 0
This is actually a rather spectacular example of dedifferentiated liposarcoma with epithelioid/ epithelial features, a rather rare but reported phenomenon. pubmed.ncbi.nlm.nih.gov/28719466/
14.05.2025 15:28 — 👍 6 🔁 1 💬 1 📌 0Now, it turns out that she has a clinical history of retroperitoneal dedifferentiated liposarcoma, with multiple local recurrences over a decade. Here’s the MDM2 IHC, diffusely and strongly positive. FISH was also done and 100% of cells showed high level gene amplification.
14.05.2025 15:26 — 👍 3 🔁 0 💬 1 📌 0Metastatic carcinoma, obviously. A big clinical work up didn’t identify a primary tumor, and a very broad panel of site-directed markers, including neuroendocrine markers, was negative. So, yet another carcinoma of unknown primary, right?
14.05.2025 15:22 — 👍 2 🔁 0 💬 1 📌 0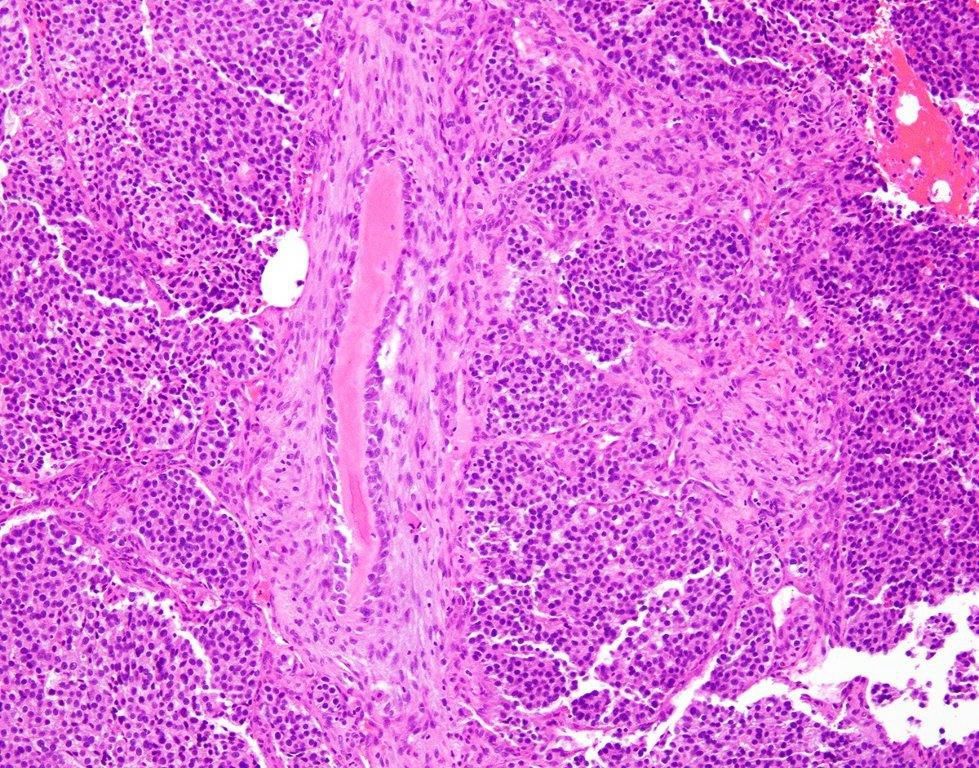
AE1/AE3
#PathSky Right femur lesion in an older woman. Diffusely keratin-positive with 3 different antibodies.
14.05.2025 15:20 — 👍 13 🔁 5 💬 1 📌 0Took me a while…
12.05.2025 16:10 — 👍 1 🔁 0 💬 0 📌 0So this truly is a superficial MPNST arising in a neurofibroma (an almost always wrong dx!) If you’re wondering, absent EED/SUZ12 mutations explain normal H3K27me3.
08.05.2025 16:56 — 👍 6 🔁 1 💬 0 📌 0Well, although I usually try to emphasize morphology, this is one where the molecular bails us out. It showed very low TMB (unlike melanoma), had two different NF1 mutations, lacked melanoma-associated mutations (other than NF1), and had loss of CDKN2A and B.
08.05.2025 16:53 — 👍 4 🔁 1 💬 1 📌 0
SOX10
H3K27me3
SOX10- higher power

PRAME
So we’re done, right? “Spindle cell melanoma- next case”. Oddly, SOX10, however was absent in about 50% of cells, as seen in MPNST. H3K27me3 expression was retained, which doesn’t help. PRAME was negative.
08.05.2025 16:48 — 👍 3 🔁 1 💬 1 📌 0